World's most ancient public health problem
Maternal mortality rates have remained stubbornly static over the past 8 years, and in some countries, from the United States to Venezuela, they have risen.
From the place I come from, in Kerala, a baby is not given a name until he/she is 28 days old. And for marginalised castes/communities, the naming ceremony is delayed to 90 days. I never really questioned as to why this was the case. I let it become a ritual system until I overheard a conversation between some of our family members. This was mainly because the chances of a baby surviving was very low in our previous times. So our forefathers temporarily delayed the naming ceremony to avoid the emotional downpour if things go south. And for marginalised communities, the mortality rate was even more low owing to the difficult circumstances.
Knowing this reality shocked me. We might have more complex challenges facing the world right now — AI taking people’s jobs, climate change induced shock waves, food insecurities, refugee rights, future pandemics etc. But I believe that the cause of addressing maternal deaths requires the most urgency. When a mother dies during childbirth, the future dies with her.
This death happens 800 times a day. Worldwide. Once every two minutes, a mother dies from complications due to childbirth.
By the time you would have finished reading this introduction, there might have been a few maternal deaths.
It’s a remarkable irony that we’re still way off when it comes to maternal mortality rate. Even despite breakthrough progress in wide range of global challenges. AIDS medicines, contraceptives, bed nets to prevent malaria, childhood vaccines, even Tuberculosis for that matter.
If you notice the figure below, you’ll only see a 3% annual decline from 2000. We’re way off the SDG target of reaching less than 70 deaths per 100,000 live births.
It’s also a strange problem as it’s not just solved by overall economic development of the respective country. Globally, maternal mortality rates have remained stubbornly static over the past eight years, and in some countries, from the United States to Venezuela, they have risen. 2
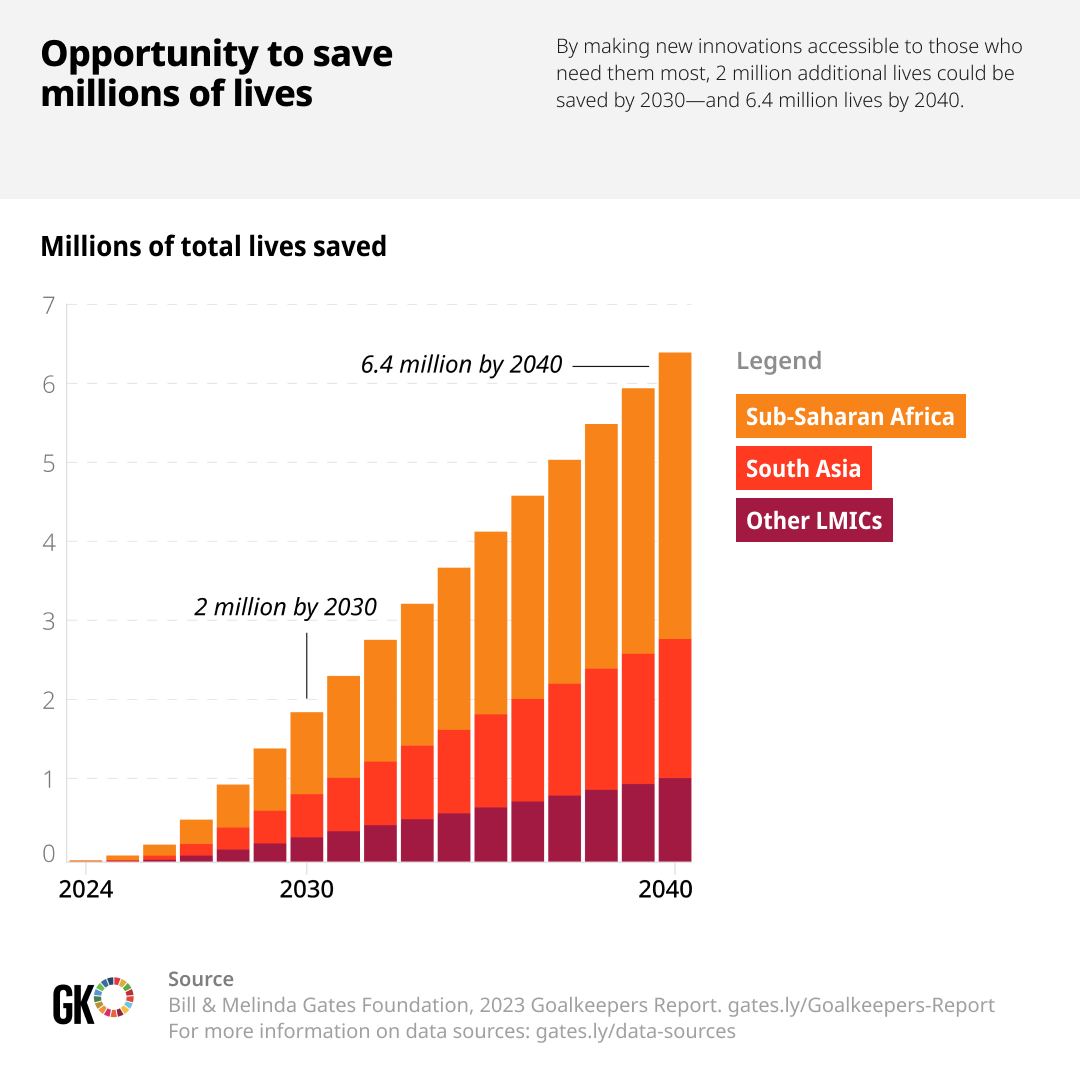
Let that sink in a bit. United States has seen a surprising rise in their MMR post COVID. The death rates of black mothers in UK and US have doubled since 1999. There is a huge opportunity for all of us to save millions of lives. If we are able to make more innovations accessible to the LMIC countries, almost 6.4 million lives could be saved by 2040.
We need innovations of all forms to tackle this. Not just technical innovations, but we need systemic innovations too. At Noora Health, we understand the power of health education training, and how that could have a profound impact for parents and their families. Our way of tackling this challenge has been through the systemic front.


An example of how we do service walkthroughs at Noora Health
By providing the right information at the right time, the curriculum is able to help new parents and their loved ones navigate this journey. For newly delivered mothers, it could be the first days for a newborn. For an expectant mother, it could be during the entire antenatal period.

Once a patient is discharged from the hospital, it’s the family who takes care of them. By imparting health education to the family, various risks are avoided. We want to tap into this unlimited resource. This, to us, is a systemic innovation as the desire to help people we love is universal.
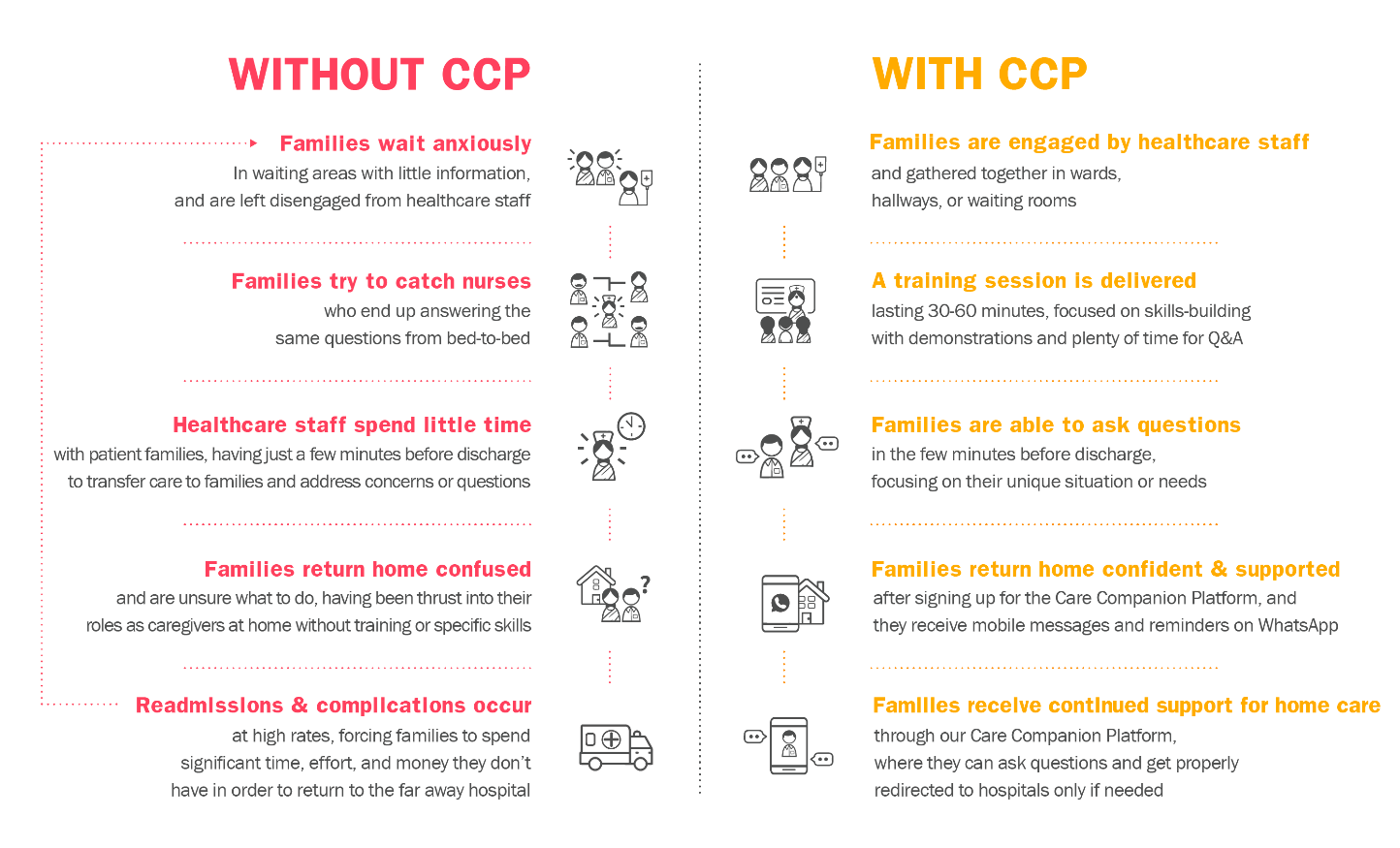
The Care Companion Program (CCP) model at Noora Health is uniquely designed around a set of principles that are known to promote behavior change, but aren’t often implemented and rarely in combination:
- Family Centered, engaging the family member vs. the patient who is often exhausted and trying to recover;
- Timely, providing caregivers what they need when they need it;
- Trust-Based, anchoring on healthcare staff who families trust,
- Skills Oriented, focusing on equipping families with actionable skills that drive health outcomes;
- Reinforcing, supporting caregivers throughout their journey from the hospital to home, not just at one time.

After leaving healthcare facilities, caregivers have access to the Noora-managed Care Companion Platform, which helps reinforce and supplement the skills and information received. Caregivers sign-up at the hospital, and then receive tailored information at scheduled points in time, including reminders and new content, most often via WhatsApp.
The Platform also provides on-demand support. Caregivers can ask questions that are fielded by Noora’s clinical team of nurses, who either clarify or supplement behavior change advice (e.g., steps for wound care, diet advice for diabetics), or provide advice on when symptoms warrant a healthcare facility visit.
While this level of support may seem daunting to provide at scale, 95% of the questions received can be answered from a bank of Frequently Asked Questions and only 5% require escalation to our team of doctors and specialists.
In this way, by looking at health education through a more systemic lens, we’re able to provide crucial information for the caregivers at each and every phase of their journey.