Healthcare
How might we enable patients to overcome preventable medical conditions?
A peek into the building of Remote Engagement Service (Bangladesh), a digital health education and support service
Imagine being a young mother-to-be, living in a remote village in Bangladesh, eagerly awaiting the birth of your child. You make the long journey to the nearest hospital for a routine check-up, filled with excitement. But as you leave, a sense of uncertainty weighs heavy – how can you ensure you'll have the knowledge and support to care for your newborn properly?
For millions of marginalised patients and caregivers across Bangladesh, this is a harsh reality. Overstretched public health systems mean many leave healthcare facilities unprepared, risking preventable complications due to a lack of essential care knowledge.
But what if a simple technological solution could bridge that gap? A digital lifeline providing vital health education and support directly to those who need it most?
Over the past 30 months, my team has poured our heart, soul, and countless hours into developing just that – a Remote Engagement Service (RES) using accessible channels like WhatsApp and voice calls. And the impact has been lifesaving.
In this essay, I'll take you on the journey of Rabeya, that young expectant mother, and share the insights gained from our efforts with RES Bangladesh—

While Rabeya eagerly waits for the doctor's appointment, she participates in the Care Companion Program, a health education service conducted by the nurses. Through simple language, the nurses provide guidance about the importance of nutrition, routine check-ups and self-care.

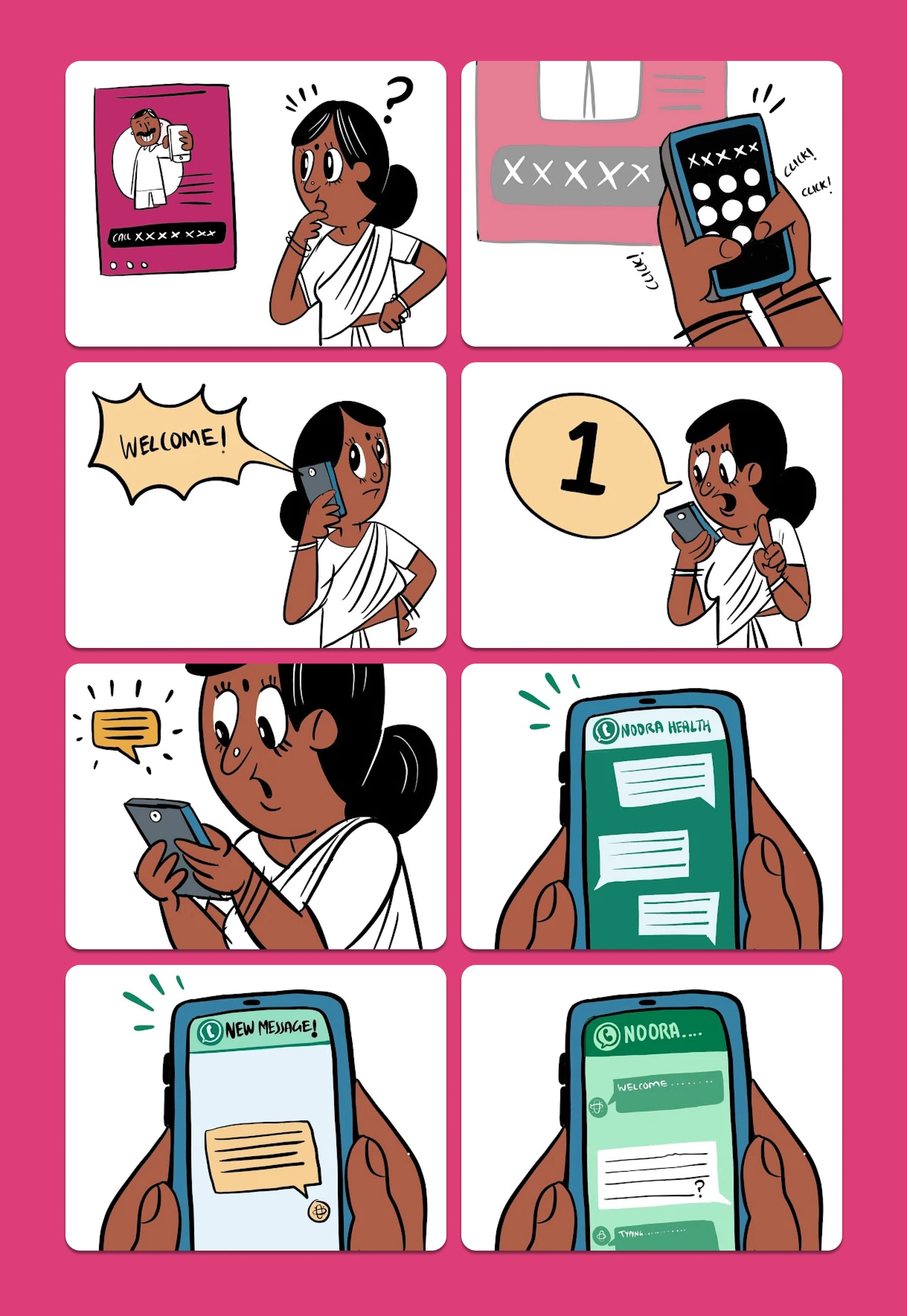
At the end of the hospital session, the nurse encourages Rabeya to subscribe to RES either through a QR code, or by directly calling the phone number.

Rabeya is onboarded to the service through a simple three-step process. She selects the campaign for expectant mothers, as well as her preferred medium (in this case, she chooses Whatsapp over a voice call service).

Once onboarded, she is gently nudged to enter her expected due date on Whatsapp. The RES service gets personalised based on this crucial timing.
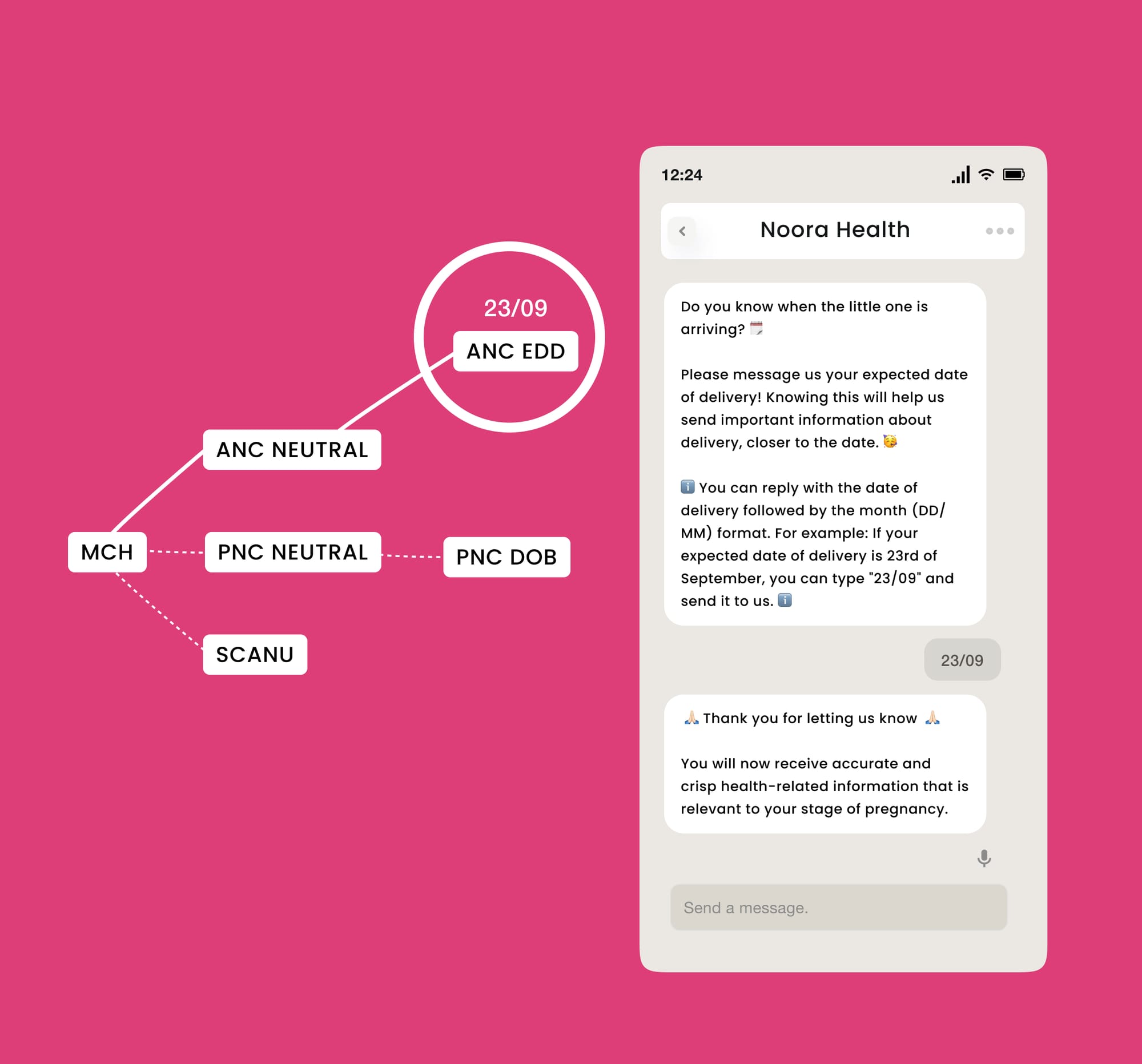

As an expectant mother, Rabeya is guided towards doing her regular pregnancy checkups from nearby facilities. She is also reminded to take her iron and folic acid tablets on time.
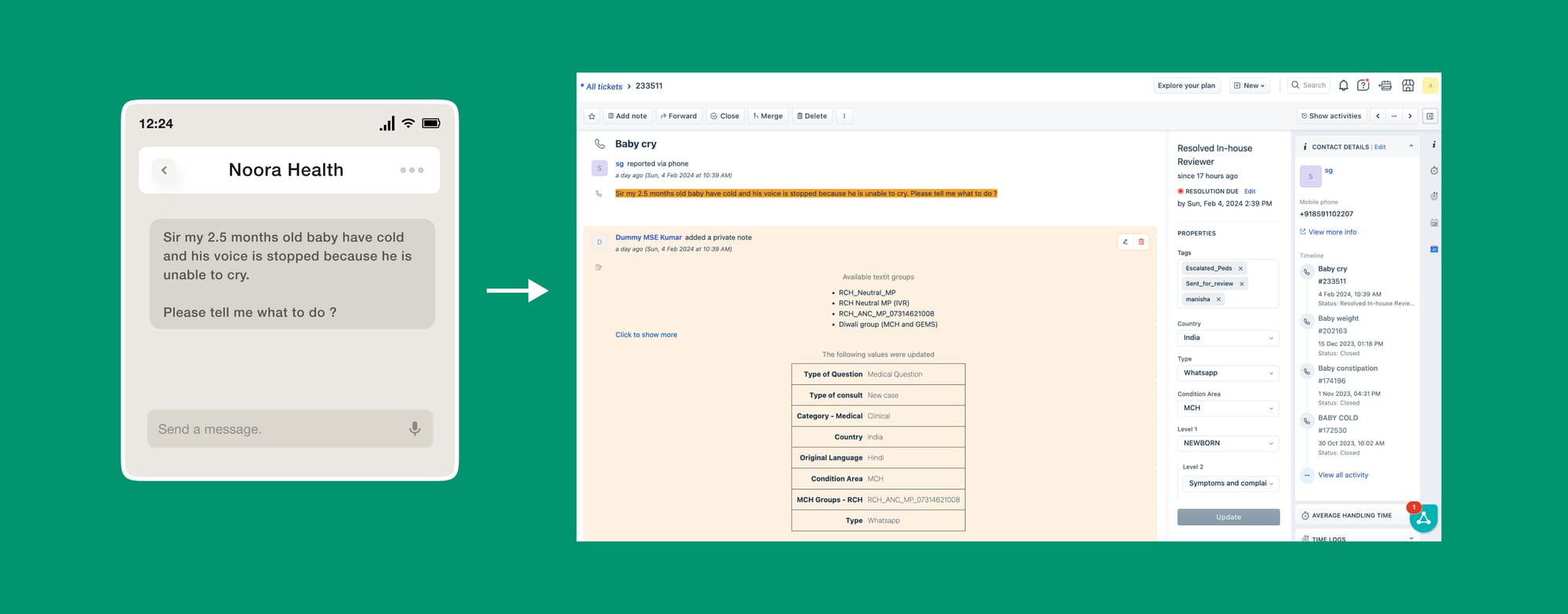
As she starts learning about various key topics, she starts asking questions surrounding her pregnancy. One day, she notices some signs in her body and remembers to seek help from the service.
In this way, she receives health support from clinical experts such as nurses and doctor as and when needed from the comfort of her home.

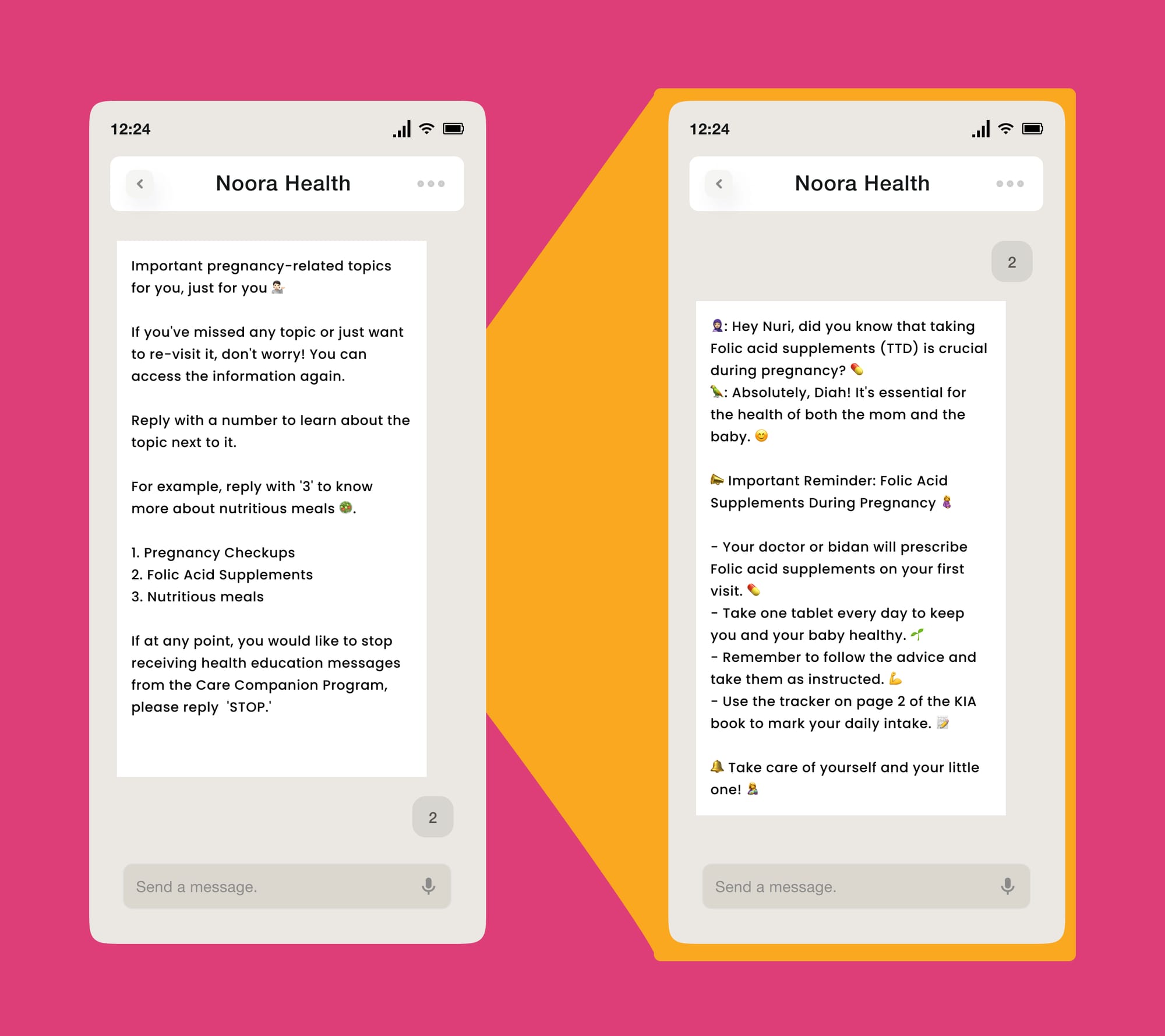
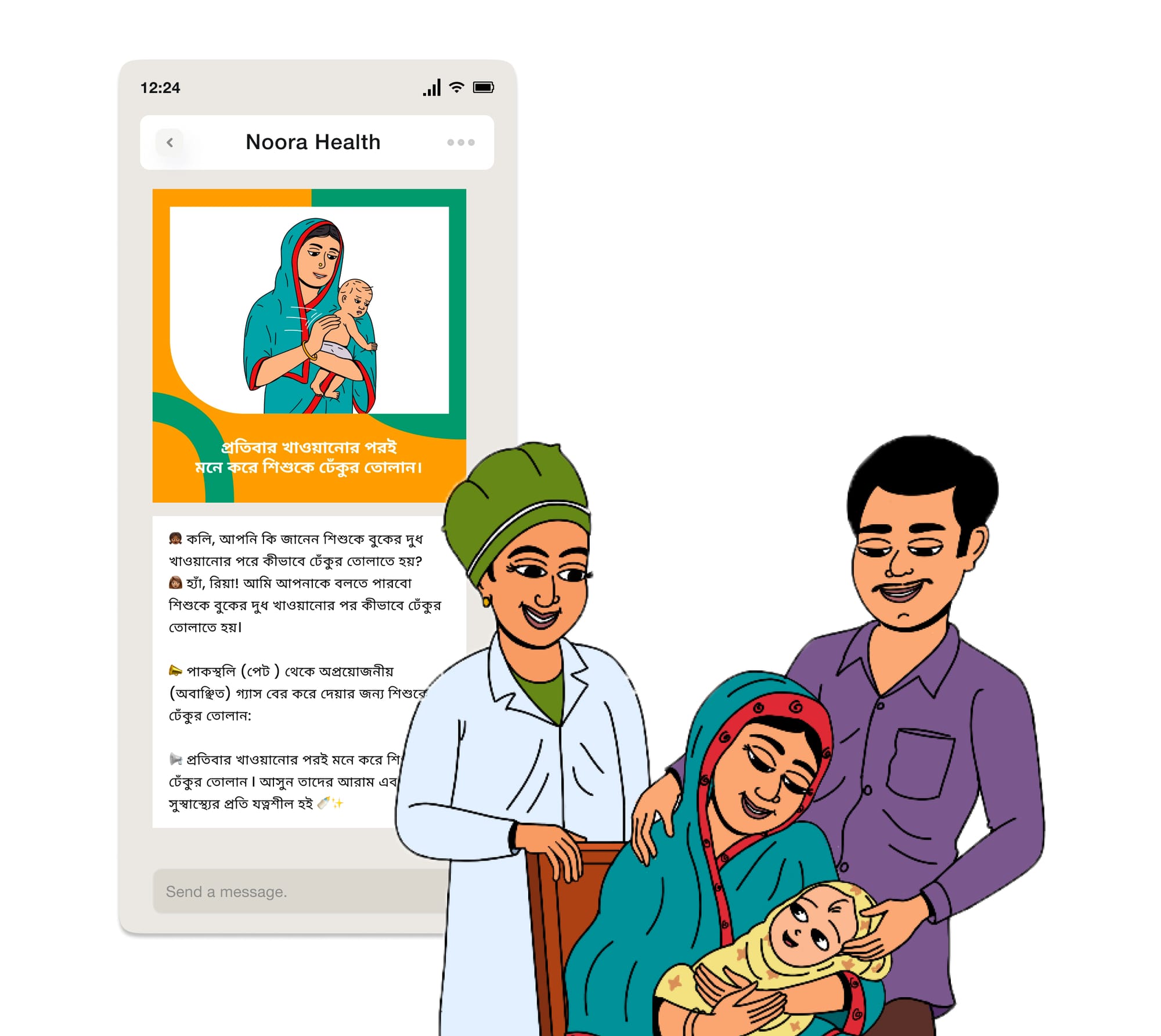
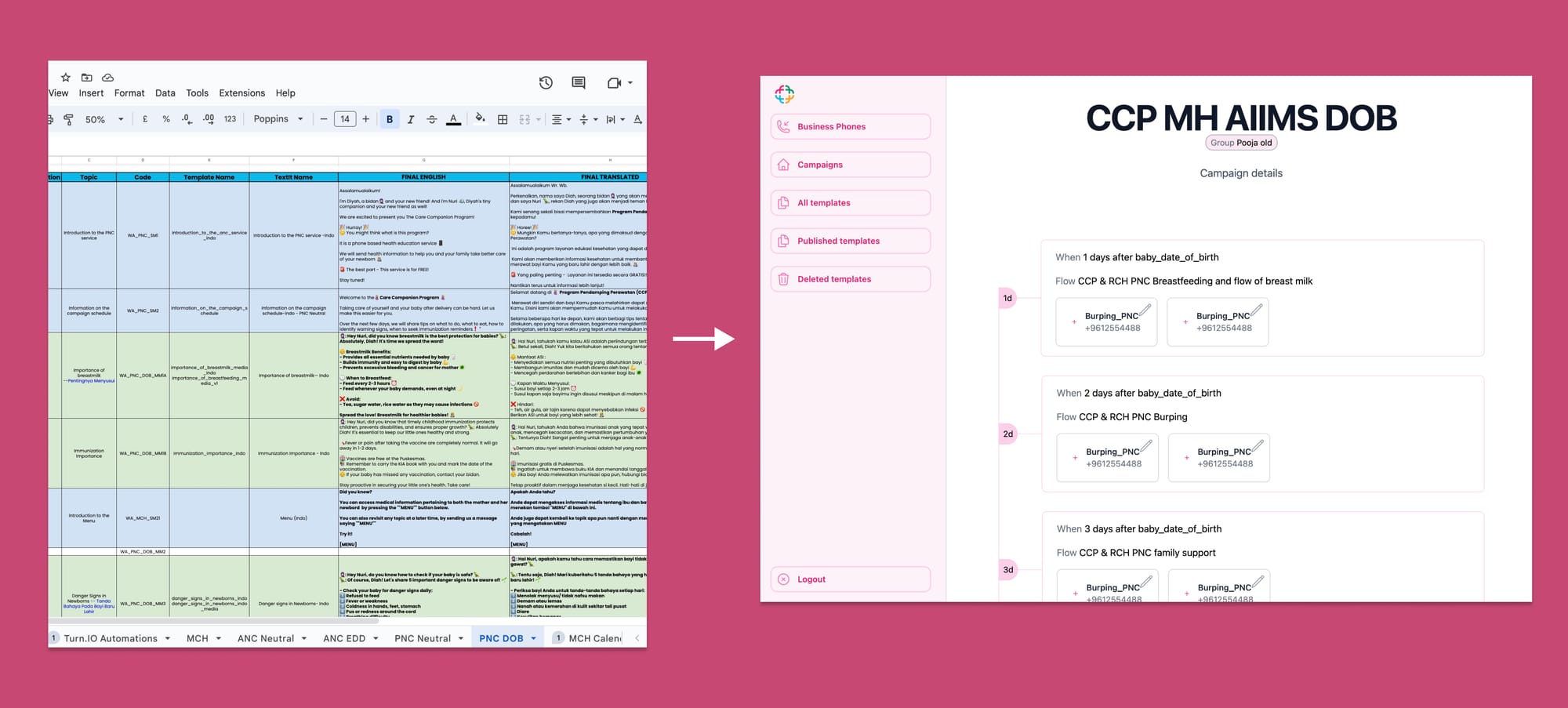
Rich media is used liberally to reinforce key health topics and to aid in retention
As shown from the journey of Rabeya, these are the core features of RES:
- Availability across multiple modalities: WA (scheduled messages, chatbot, and live chat), Voice (IVRS), Teletraining (live calls)
- Availability across multiple condition areas: MCH (Maternal and Child Health), NCD (Non Communicable Diseases), Cardiovascular, TB (Tuberculosis), General Surgery/Medicine
- Human-in-the-loop AI health responses: Only medical experts provide health responses. By leveraging LLMs, responses are served in a reliable, accurate and efficient manner
- Provides Behavior Change Communications: Both instructional and narrative styles of content, rich media (images, gifs, short-videos)
- Customized to stage and severity of need
Journey behind building RES
I’ll go one level deeper into the process followed—
Phases
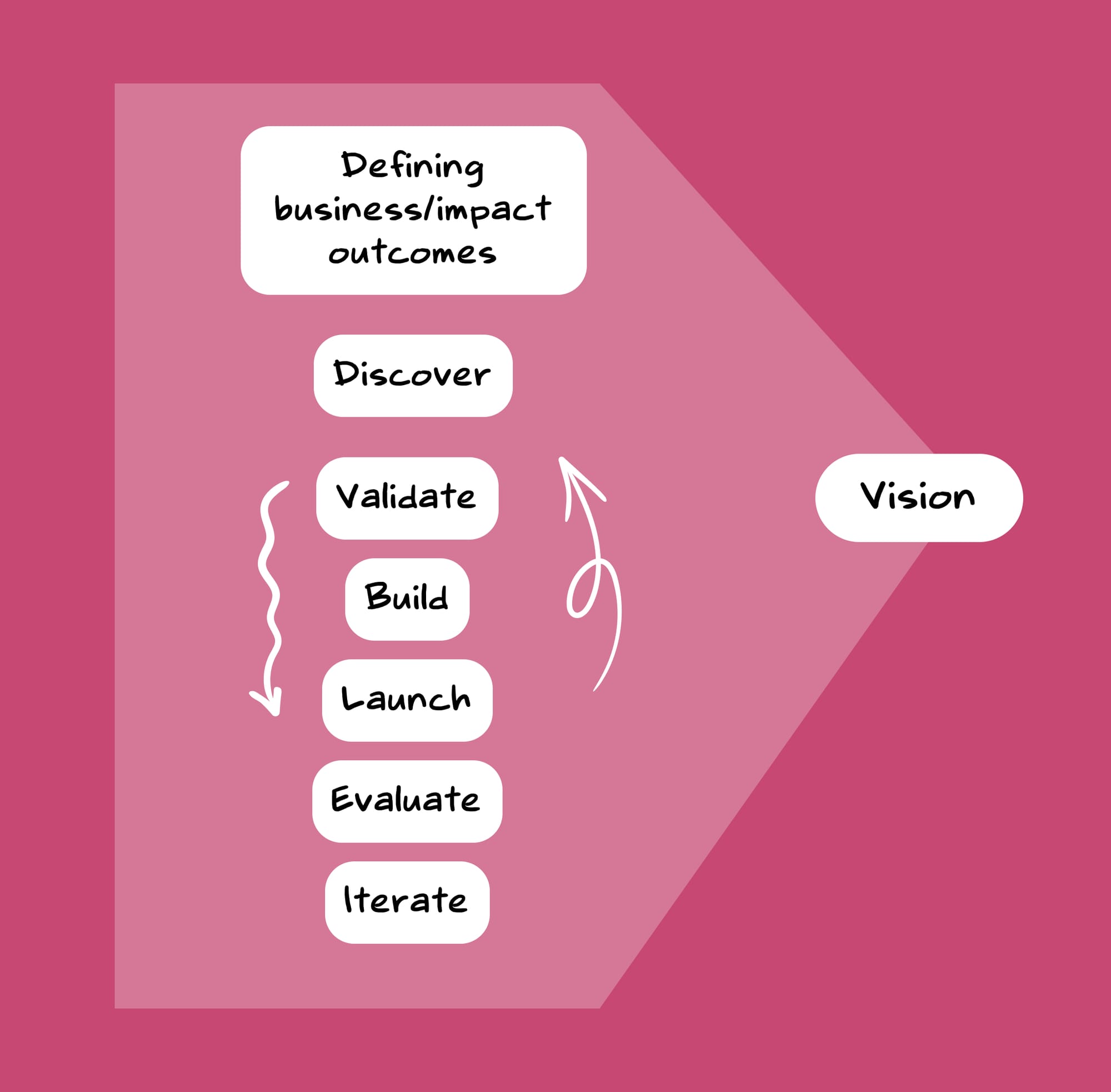
One—Defining Business/Impact Outcomes
The phases such as Defining Business Outcomes, Discovery, Validation, Building, and Launching might seem like disparate blocks, but they were all tied together by the vision. This vision serves as the connecting tissue, helping move the pieces together seamlessly, like a well-oiled engine without any jitters.
As a Business-to-Government-to-Consumer (B2G2C) model, we aimed to support Bangladesh government's health initiatives were focused on reducing the maternal mortality rate (MMR) and infant mortality rate (IMR). Bangladesh had roughly ~157 maternal deaths per 100,000 live births. To provide a benchmark, the Netherlands has ~4 maternal deaths per 100,000 live births. Noora Health's pitch to the government was to establish family caregiving as a standard of care, thereby reducing the MMR and IMR rates through the intervention.
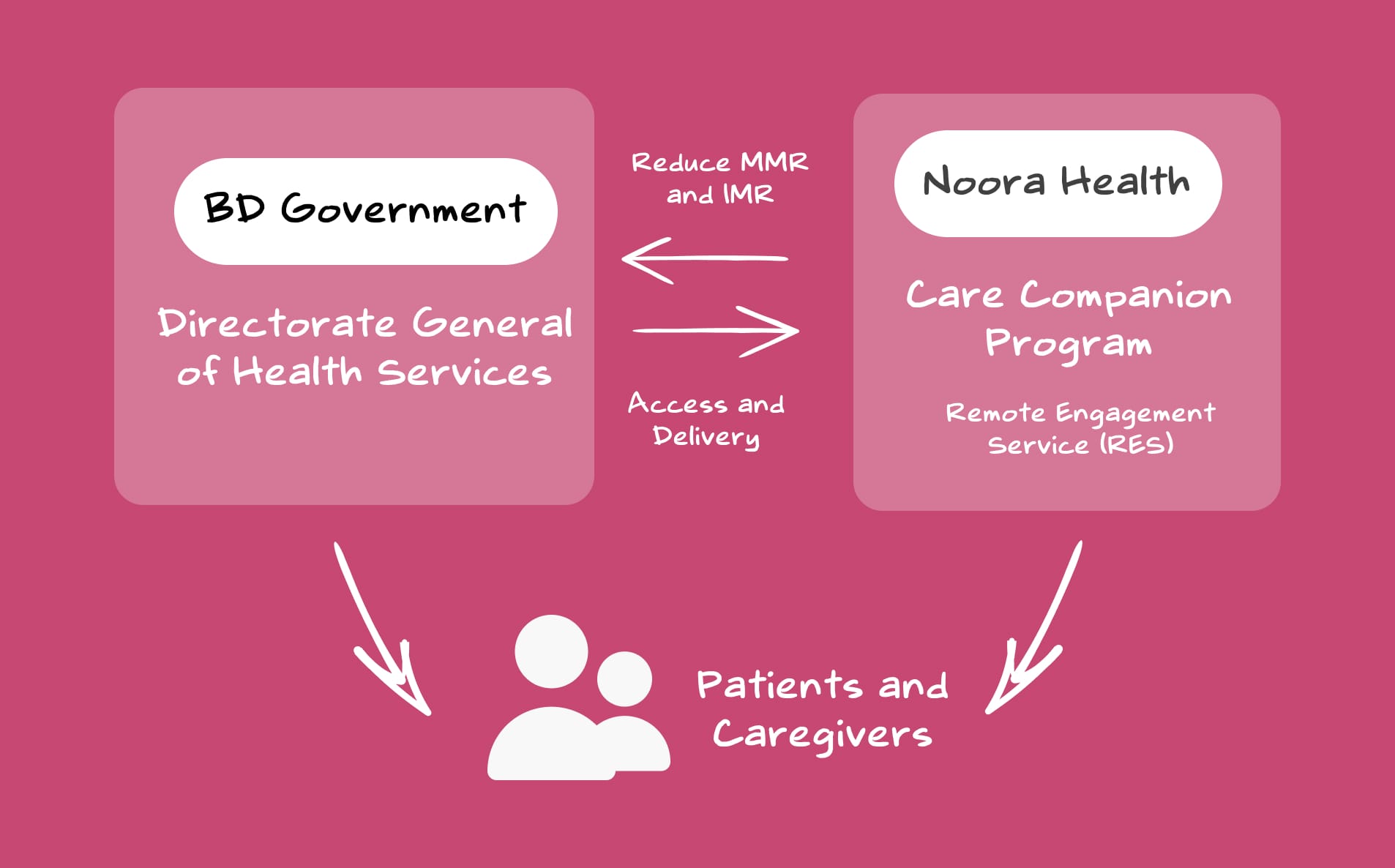
We got into our first MoU with the BD Health Ministry to pilot, gain evidence, and to integrate the program into the public health systems. That’s how we started our operation.
My initial efforts during this phase was to make RES simple and easy to remember. To reduce the complexity in the communication, and to revive and evangelise interest towards RES, I showed a vision for RES BD—Every user overcomes any preventable medical condition digitally. Nurses were also trained to communicate RES in a simplified manner as—'Health education for you and your baby'.
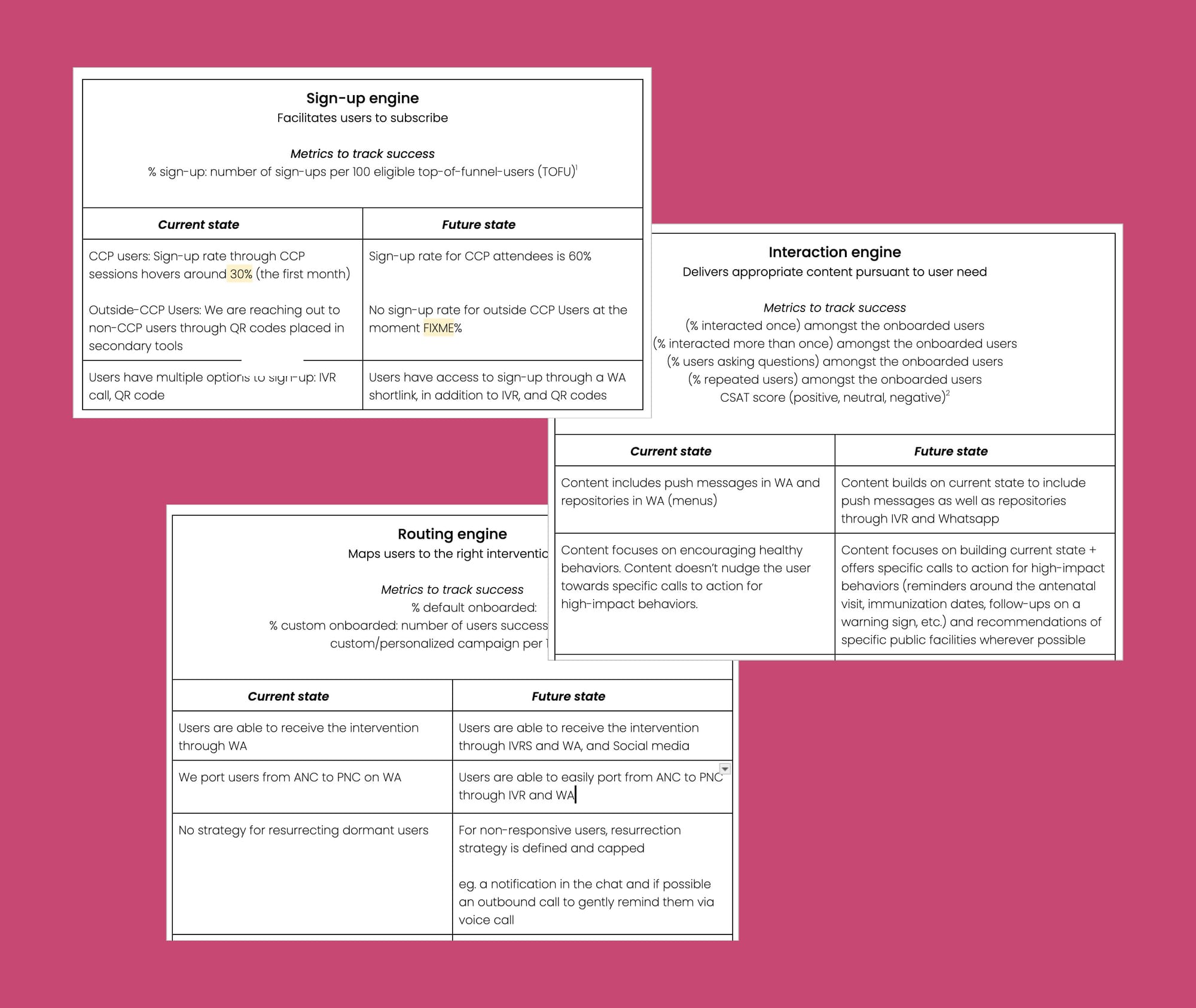
To make the direction of the vision even clearer, I worked closely with the Head of Product to break down the complex roadmap of RES into a simpler, more digestible format for all team members.
Discovery Phase
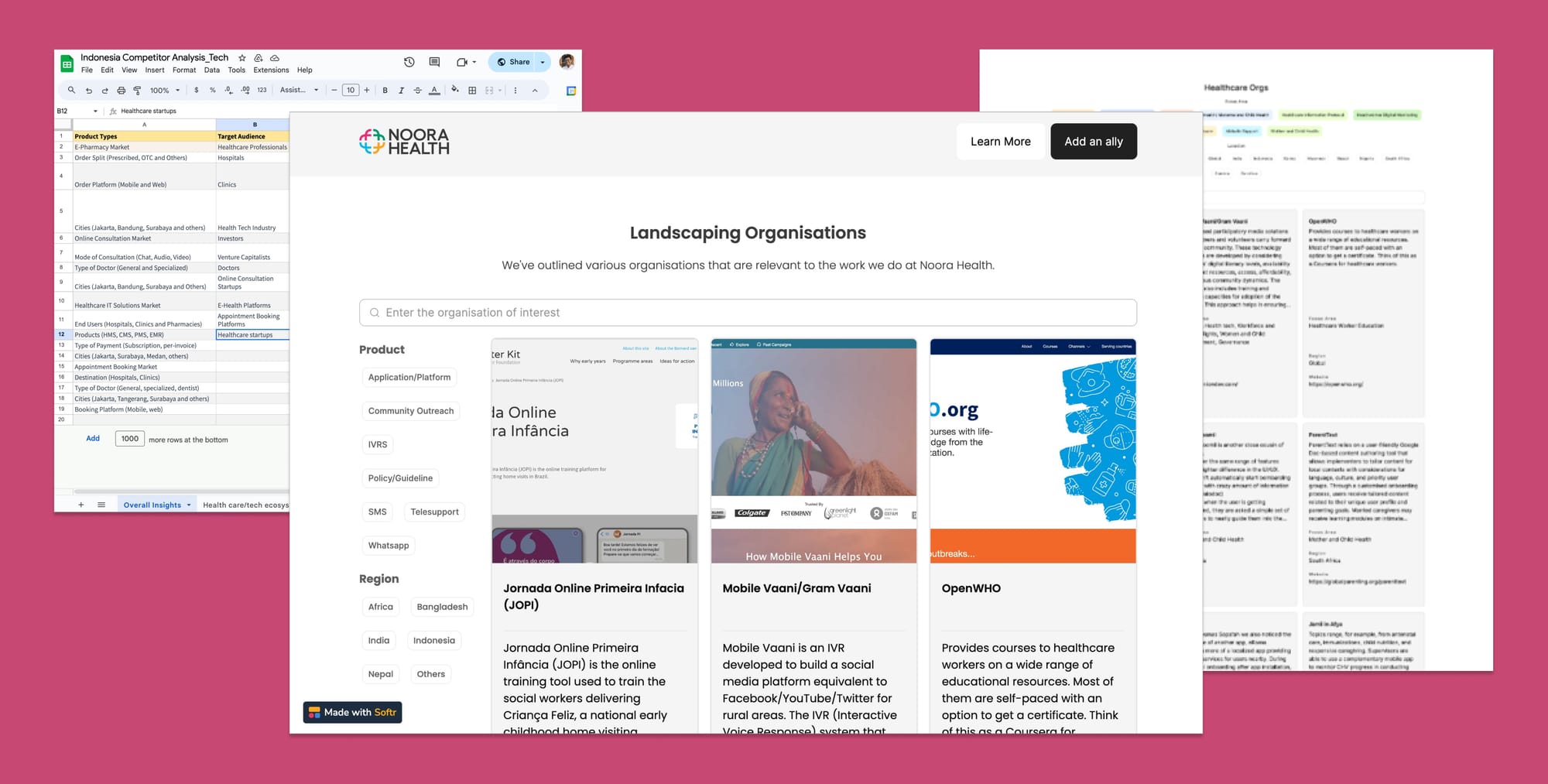
Recognising that a direct replication of our previous strategies in India wouldn't suffice, we approached the situation with a fresh perspective.
My team and I explored the patient health journey across district hospitals, sub-district hospitals, and primary care centers in Bangladesh. This exploration aimed to map out how patients were accessing healthcare systems.
We were not optimising for a single user journey; rather, we addressed multiple journeys across various segments and touchpoints. Consider Rabeya's path—her experience extended far beyond that initial visit to the sub-district hospital.
Rabeya might attend her antenatal checkups at the local health complex, received home visits from community health workers, and may have even been referred to a higher-level facility for certain procedures or complications.
Each touchpoint represented a crucial opportunity to educate, empower and provide continuous support tailored to her evolving needs.
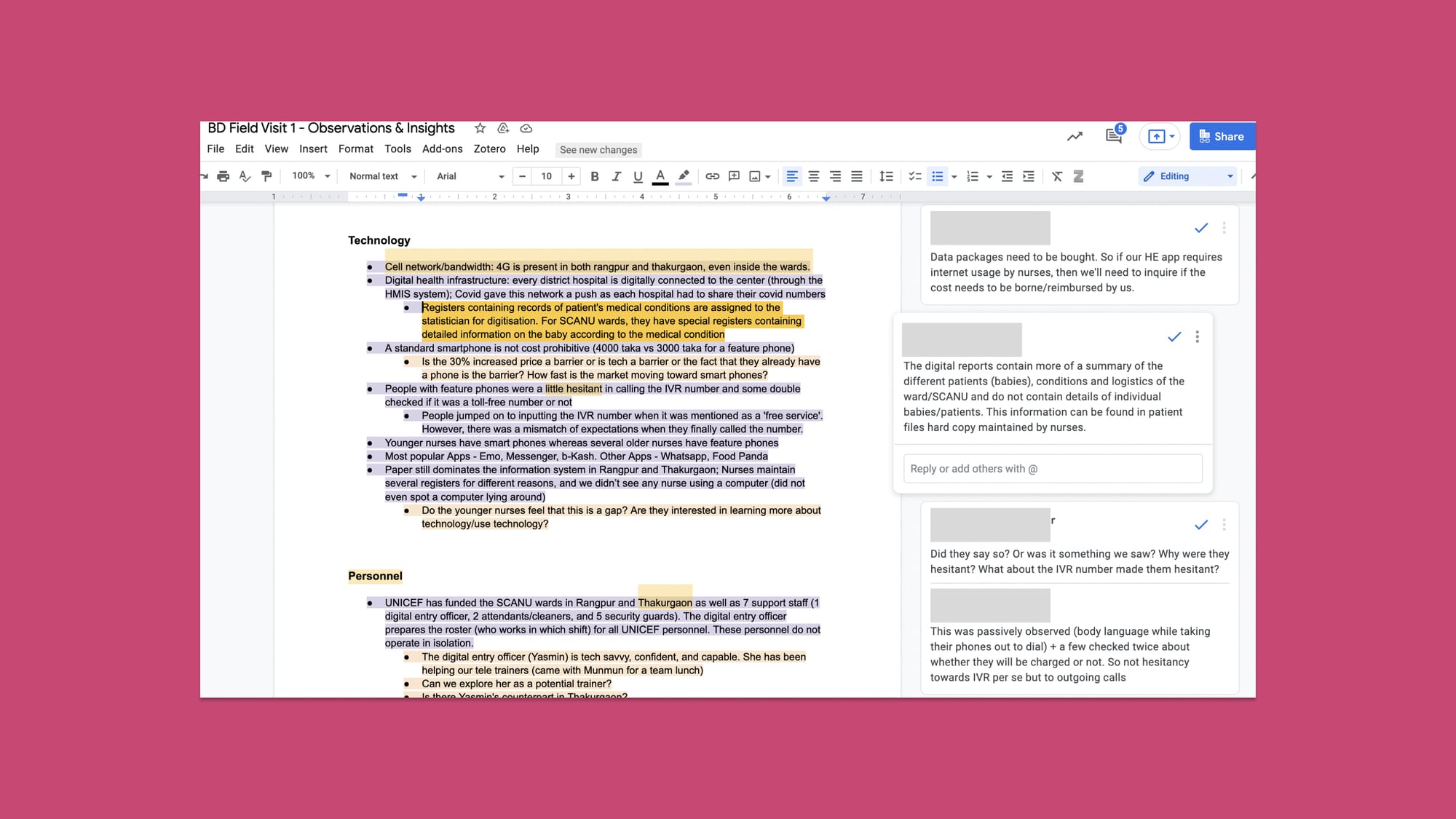
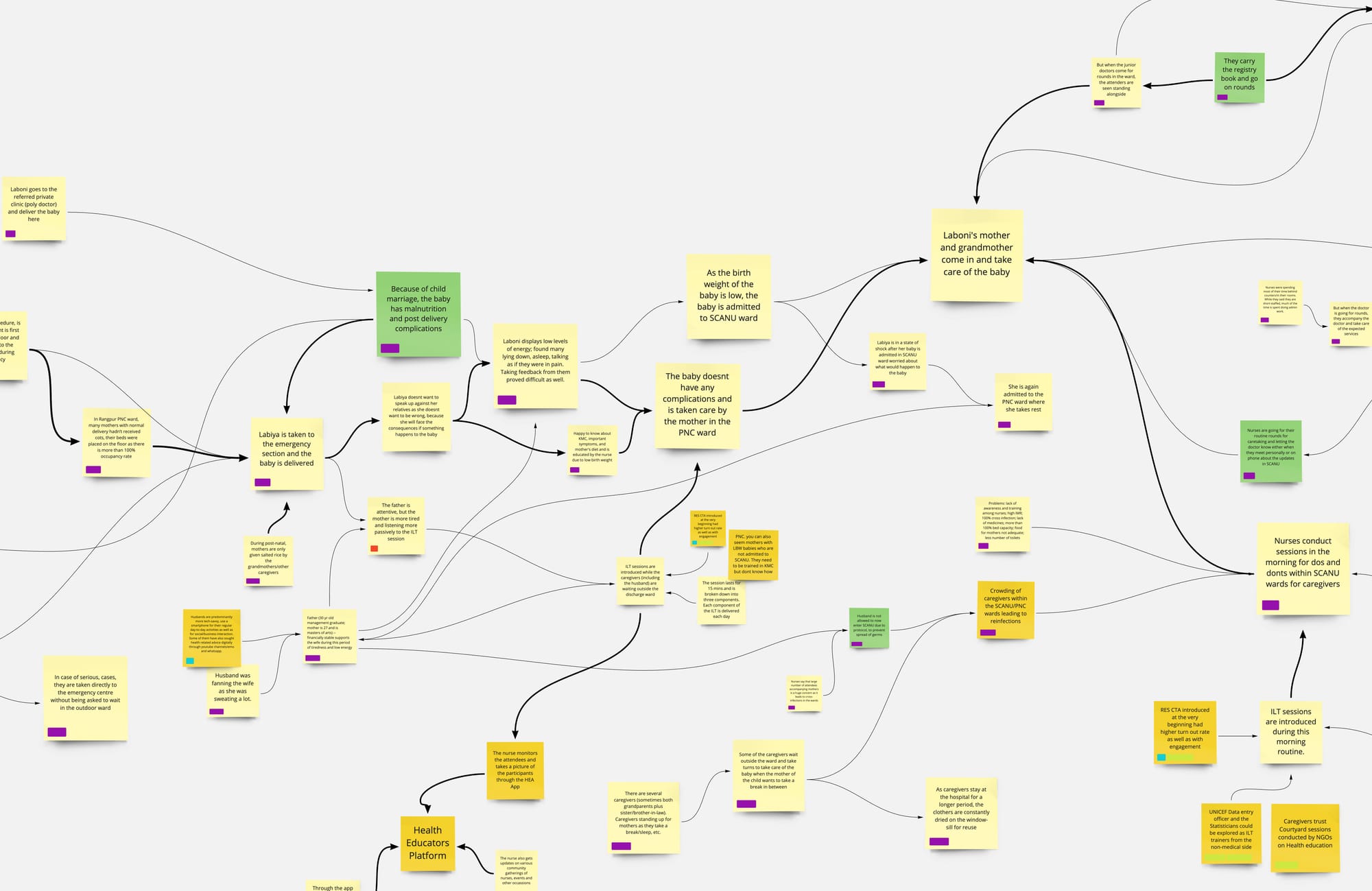
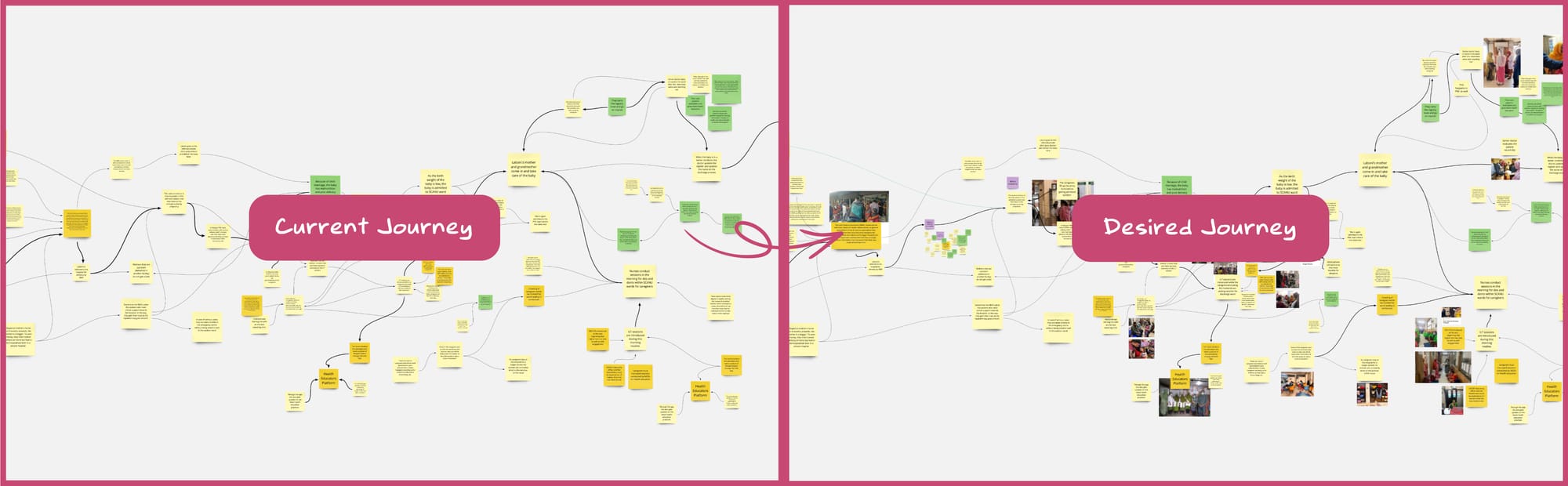
This synthesis (through affinity maps) informed the initial draft of our product requirements document, ensuring it was grounded in the diverse findings from our field and desk research. This helped us to imagine the desired journey in contrast to the current journey.

Another framework which proved to be quite useful in digesting the complexity of the multi-touchpoint user journey was the service blueprint.
Some key directions from our discovery phase:
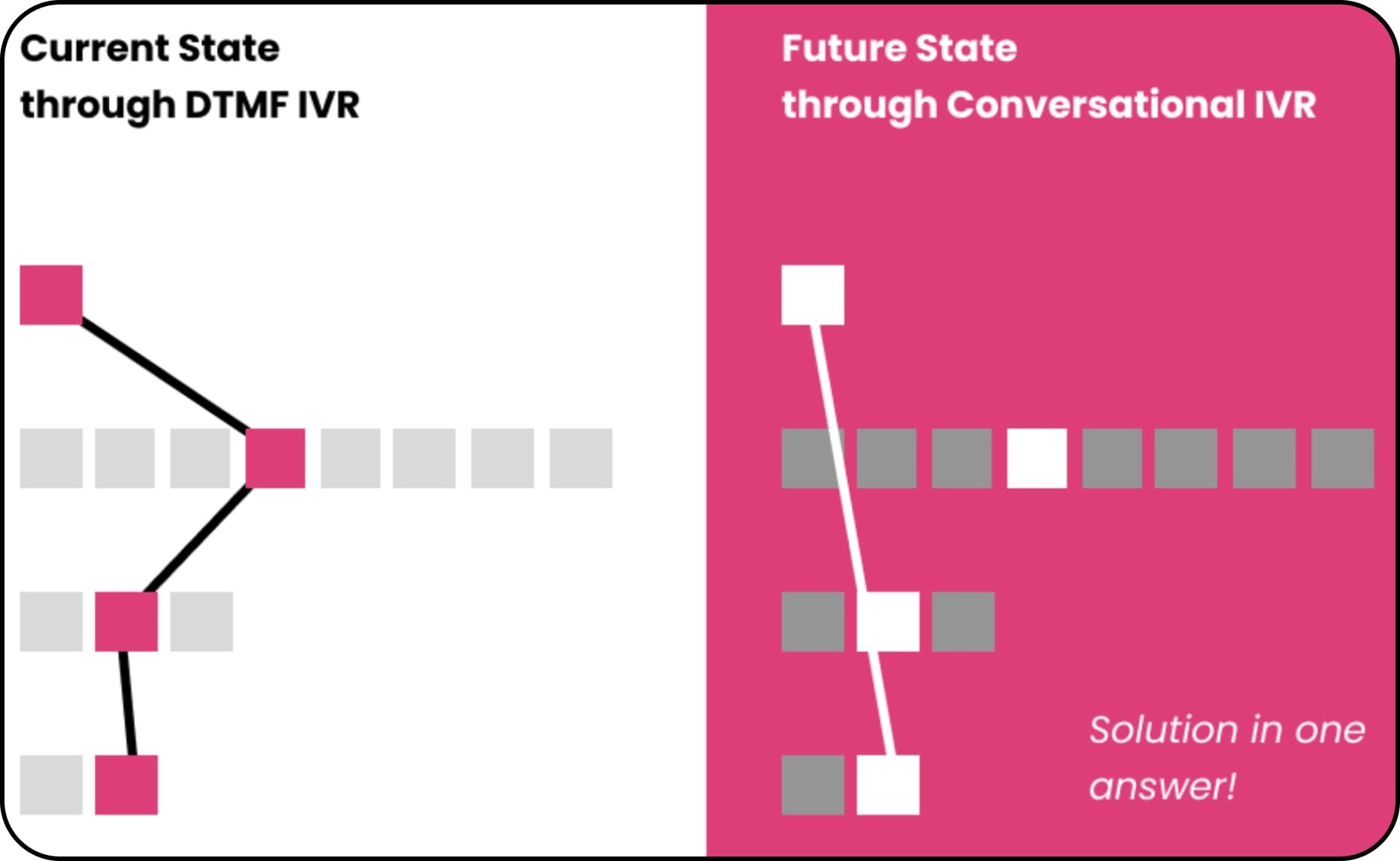
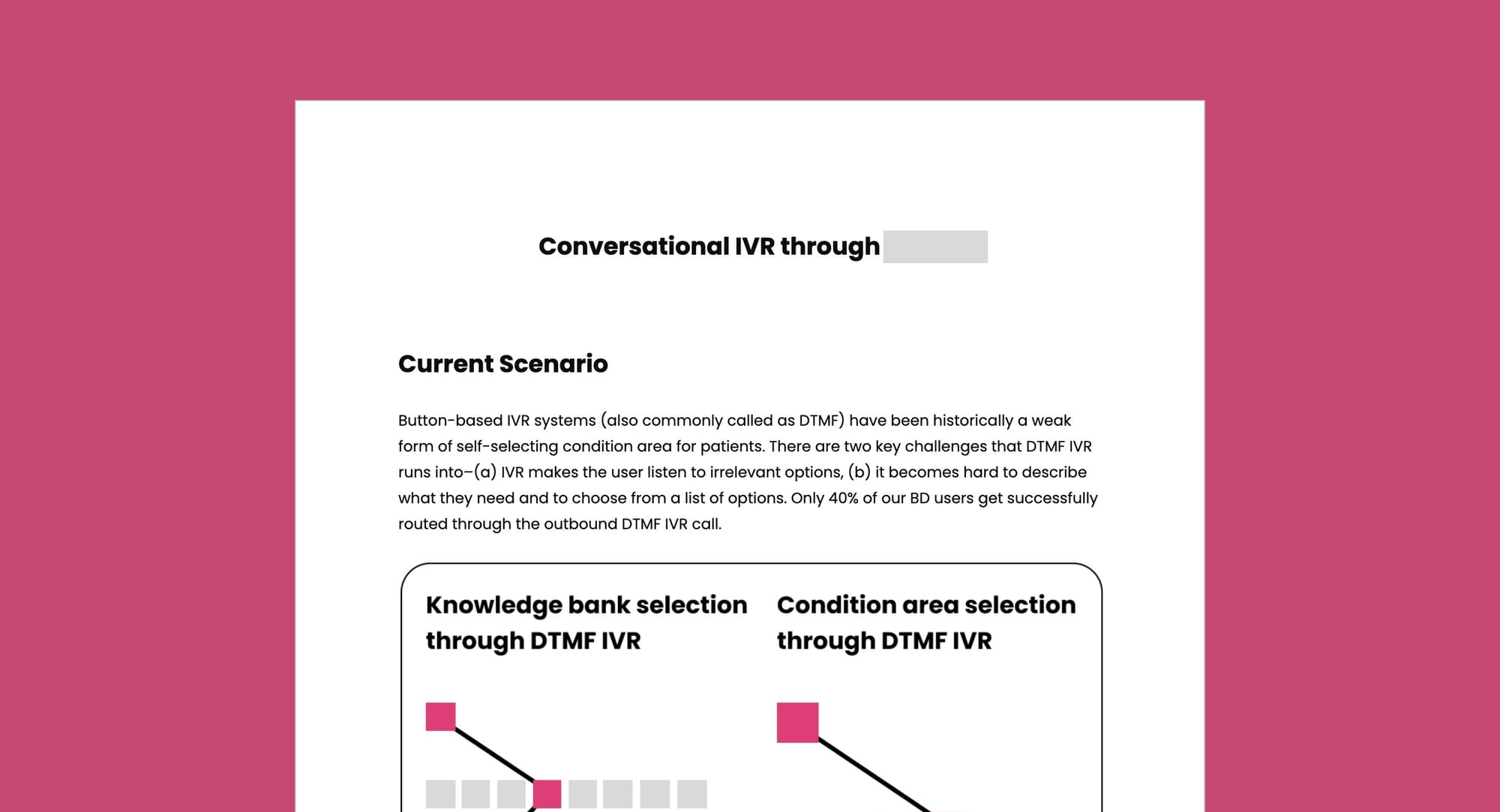
Voice calls as a primary medium—During our discovery phase, we analyzed the overall usage of smartphones among the rural populations in Bangladesh. As of last year, 41% of mobile phone users in the country had smartphones. With low WhatsApp penetration and internet usage being distributed among various platforms like Facebook and Emo, Interactive Voice Response (IVR) was chosen as the primary medium for our RES service. This decision was supported by our field observations and corroborated by reports, which indicated that often only one smartphone is available per family in rural areas (The Business Standard) (GSMA).
Timing our service around date of discharge—We designed our RES service to start immediately after a high-risk baby is discharged from the hospital, typically after 7-9 days. This timing aligns with one of our core design principles: to provide the right information at the right time. We adopted a similar strategy of timing our service while designing for diabetes patients, surgical care, newly delivered mothers etc.
Contextualisation and personalisation of the messages—RES campaigns were made more personalised to the geography they served. We adopted a more conversational format mixing curative, and promotive themes for behaviour change. We went on to also hire country specific teams across the Health Communications, Medical Strategy as well as Media/Film to ensure the content was adapted to the context.

All these guidelines and features were depicted in the product requirements doc that served as a means of garnering consensus, providing clarity to the respective engineering and design teams.
Validation Phase
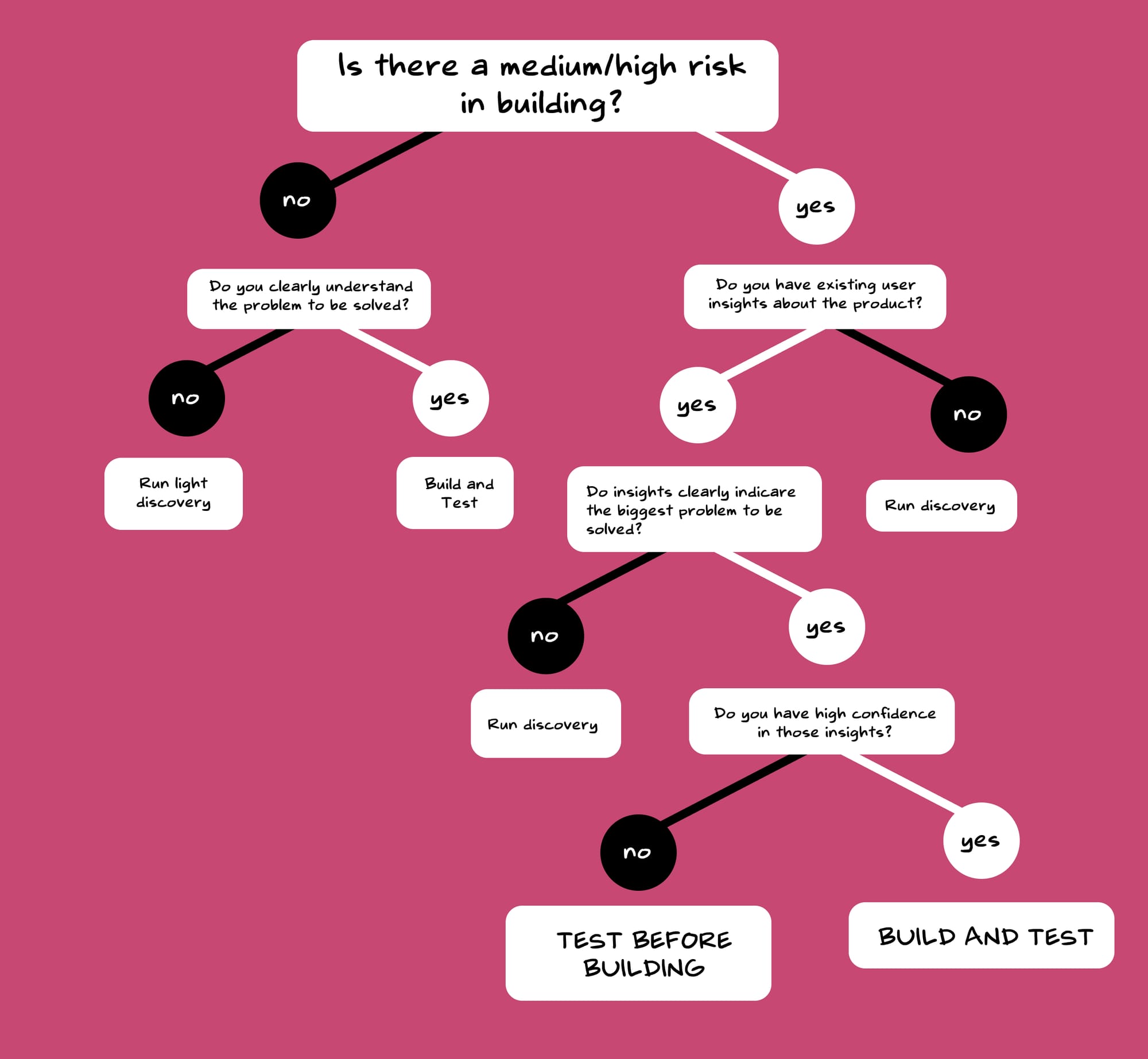
Should we build and then test? Or should we test and then build?
When facing this dilemma of whether to—build and then test a product or to test and then build, our approach varied based on the situation. As we always dealt with the trifecta of scope, time and effort, we needed a more structured approach to deal with these decisions. For more 'risky' features, we designed a lightweight pilot version first to test the concept in a controlled, manageable way. However, if the associated risks were minimal, we chose to launch first and then validate the feasibility afterwards as shown below—
Build/Launch Phase
Our product development process blended elements of both waterfall and agile methodologies, particularly crucial in the healthcare sector where careful planning of user-facing releases is imperative.
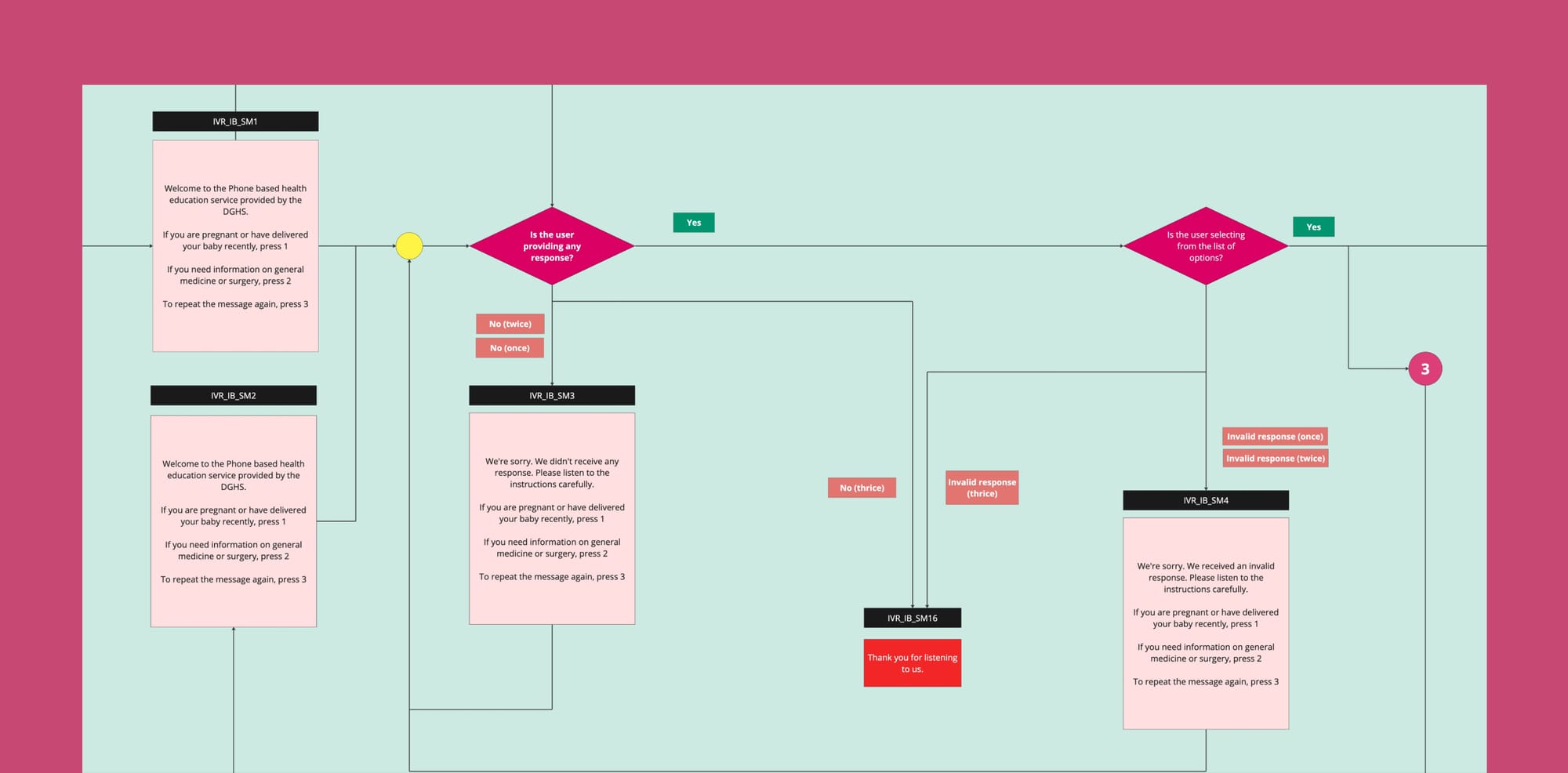
We methodically rolled out features over a 2.5-year timeline, carefully managing the evolution and growth of the service. The roadmap for what needed to be built was articulated in a detailed service map (as shown below), which facilitated collaborative feedback from all stakeholders. This ensured smooth transitions during technical handoffs, reducing risks and enhancing the effectiveness of our launches.
Evaluate Phase
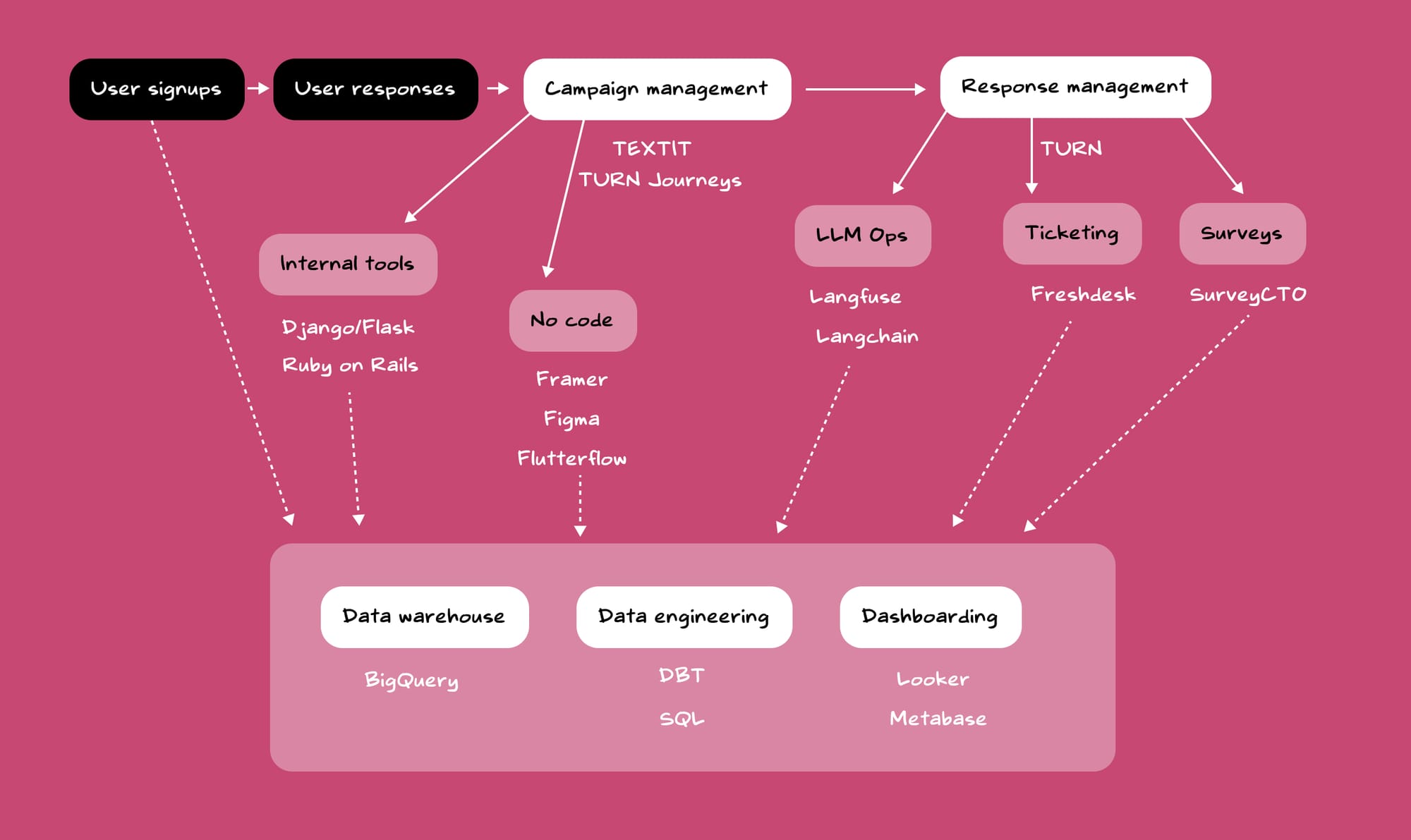
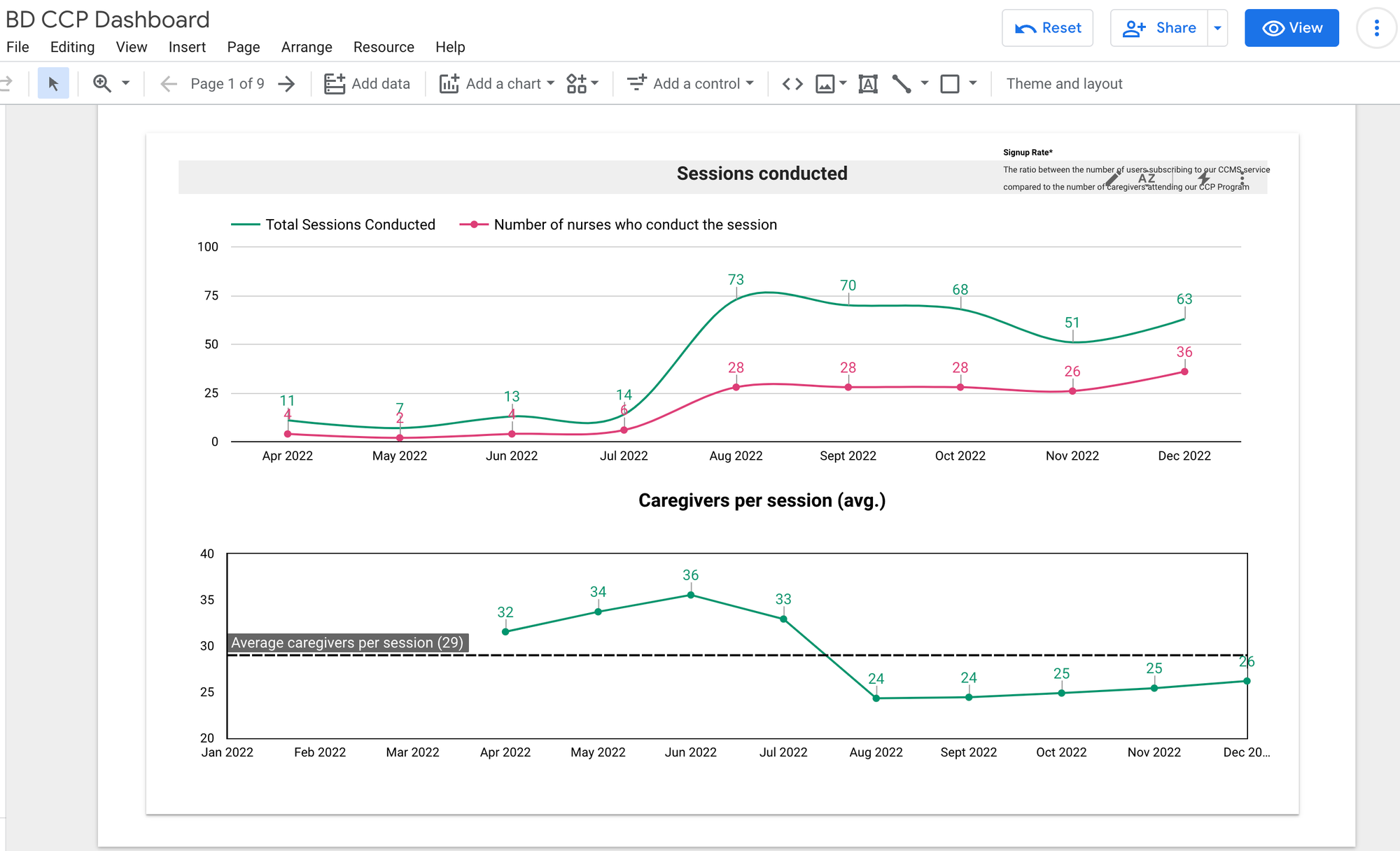
Before we evaluated, we didn't have proper systems to evaluate. When we started, we lacked a centralised product dashboard integrating data from various sources.
Setting up systems for data-led evaluations
To support the tech team, I created early prototypes of the dashboard to demonstrate our requirements to the tech team. The visual prototypes proved to be useful for kickstarting conversations around the dashboard and gaining momentum to push it forward.
After diagnosing, and identifying the gaps, the data engineering team established pipelines, warehouses and the dashboard for helping us take data-driven decisions.
Setting up systems for user-led feedback loops
To collect more insights from the field and from our users themselves using our service, we established a regular schedule of field visits for the RES team to engage directly with patients and caregivers. This allowed us to continuously gather and analyse data from various channels to better understand their needs.
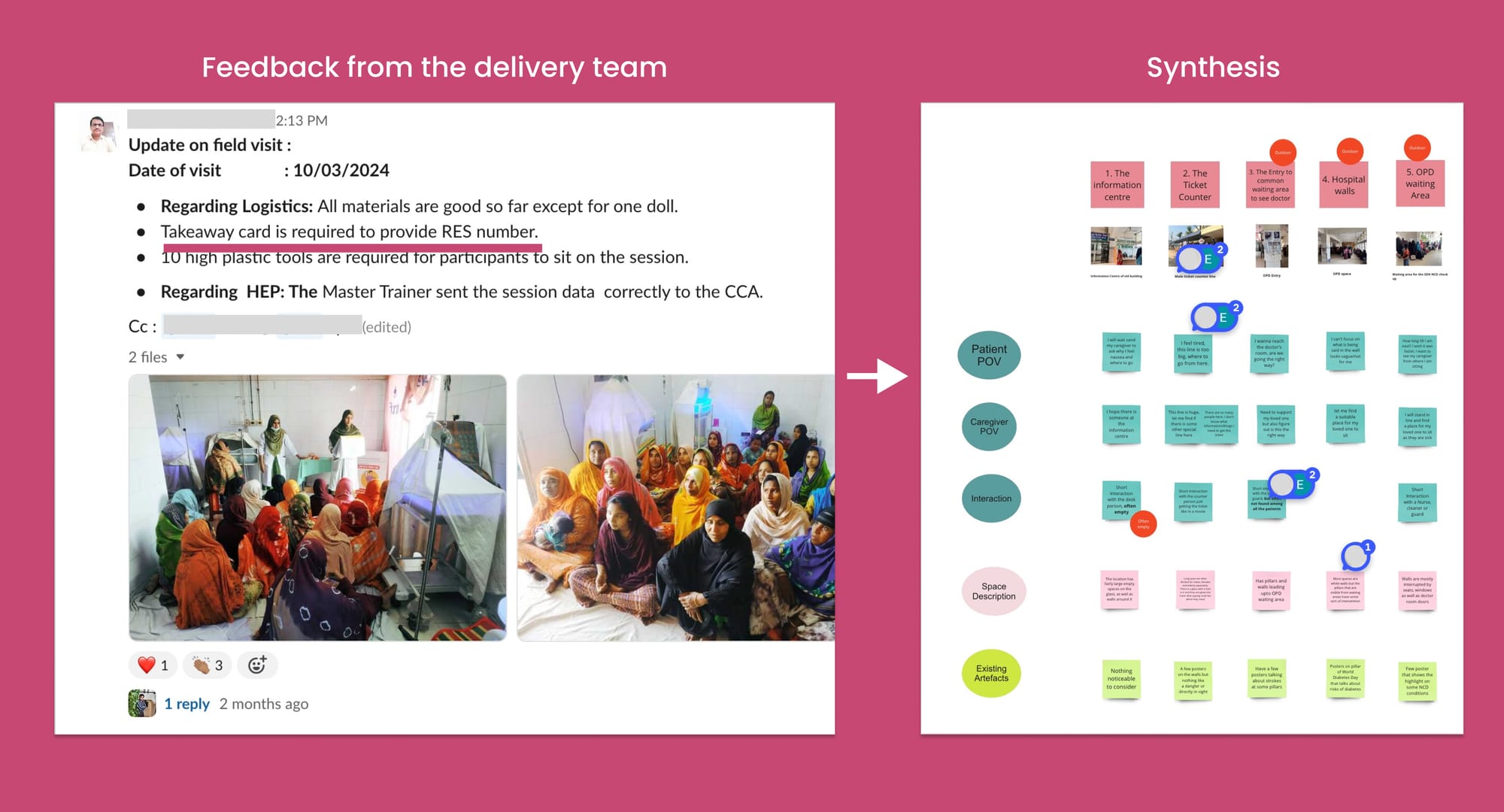
Key initiatives that I spearheaded to deepen our user-feedback loops included:
Mid-campaign support calls—These calls not only built trust with caregivers but also served as vital two-way communication channels. For instance, we discovered that 96% of our Whatsapp users read our messages, but struggled with literacy, impacting their understanding of the health-related content.
End-campaign surveys and feedback—Responses to our messages and updates from the delivery and implementation teams were crucial in synthesizing insights. On one occasion, we learned that users were sharing the RES contact number using takeaway cards among family members. This observation prompted us to redesign these cards to facilitate easier dissemination among patients and caregivers.
Taking effective decisions—A good decision was a mix of taste, data and insights. After having set up systems to process data, systems for gaining user feedback, it became relatively easier to take crucial decisions. Taking both data and insights into the decision making process was quite crucial. In some cases, we had contradictory user viewpoints. Or in other cases, the data was quite contradictory to the user narrative.
What people say, is different from what people do, is different from what people think.
Example decision—Deciding between voice calls and Whatsapp
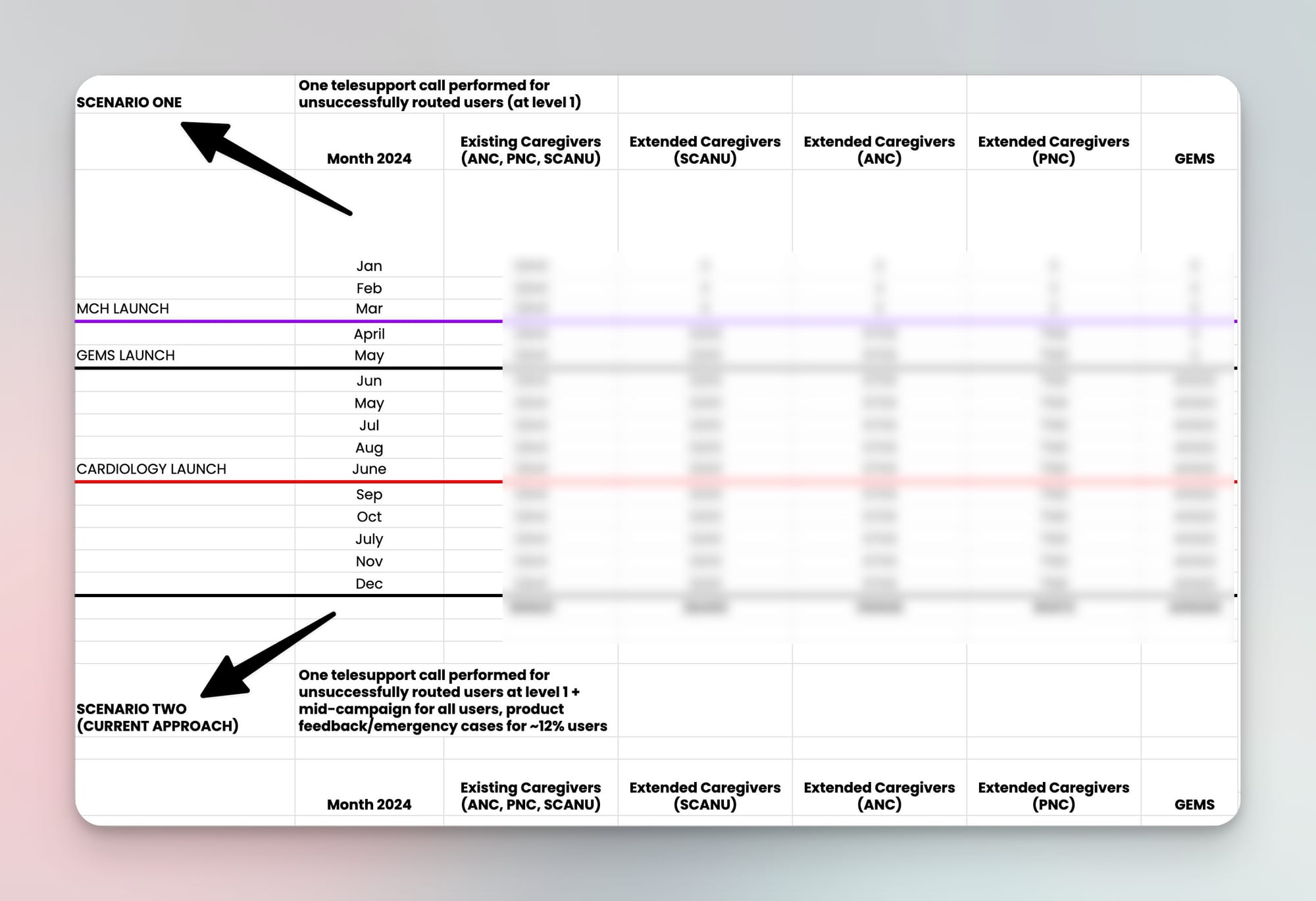
Example decision—Evaluating telesupport capacity
Iterate Phase
One of my core philosophies in product development is to view each product as a work in progress that is never truly complete. This perspective reinforces the necessity for continuous improvement, as a product is never 'done'. In managing our development cycles, I advocate for a 70% focus on enhancing existing features (exploit) and 30% on exploring new possibilities (explore). This approach ensures that while we continuously refine our product, we also remain vigilant to emerging cultural, regulatory, economic, and technological trends. Exploration is conducted through a '5C lens'—Customers, Collaborators, Competitors, Climate, and Company—to identify and integrate new opportunities into our opportunity hypothesis.
For instance, we observed a growing trend in the use of large language models (LLMs) to deliver health-related information quickly and effectively. Inspired by this development, we integrated LLMs into RES, primarily to enhance health intent recognition and support clinicians in providing faster, more accurate responses.
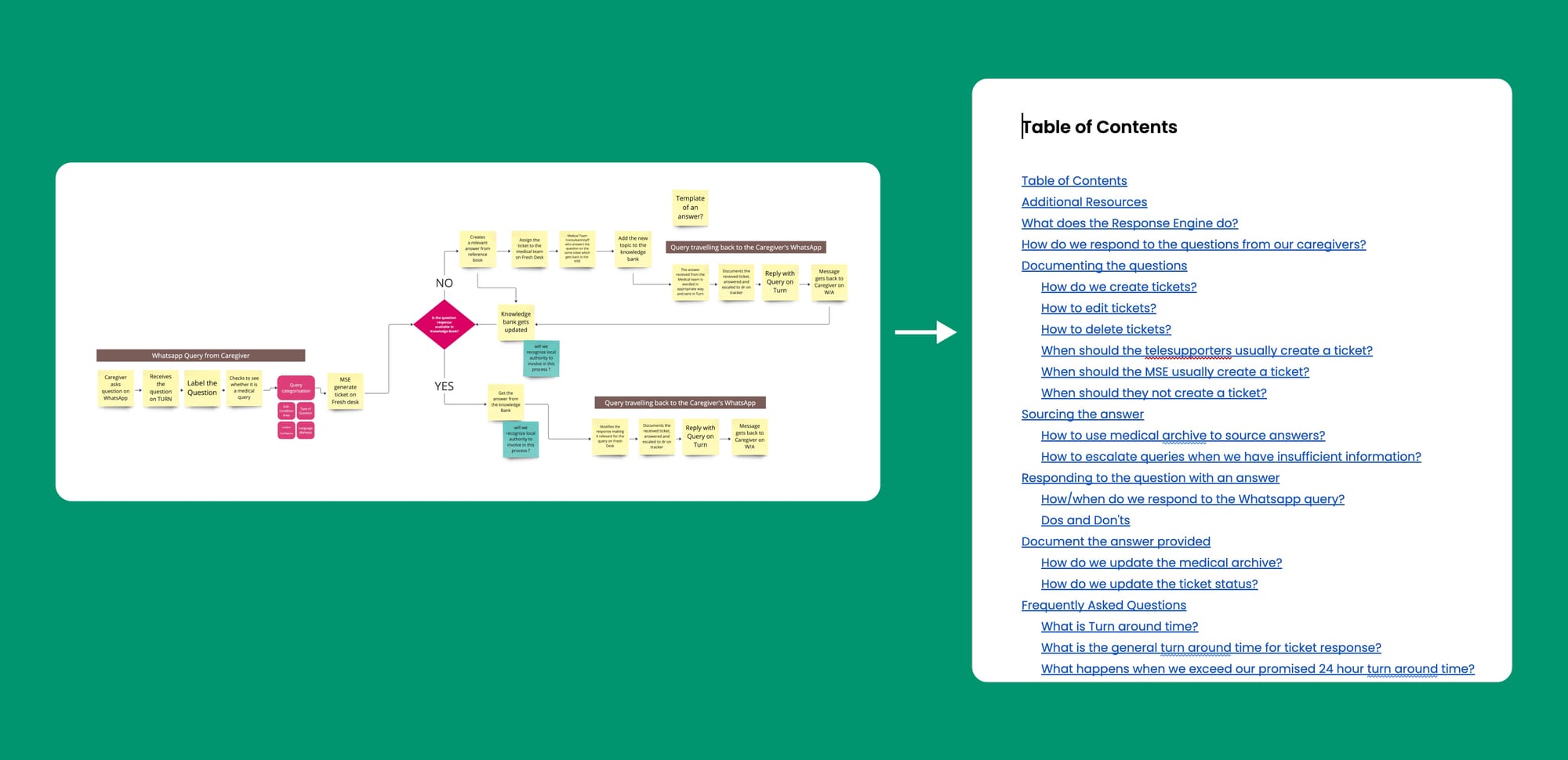
In the exploitation phase—we focused on refining our core product—we devoted considerable efforts to structuring our response system more efficiently. This involved creating knowledge banks to prevent repetitive responses and formalising protocols through standard operating procedures.
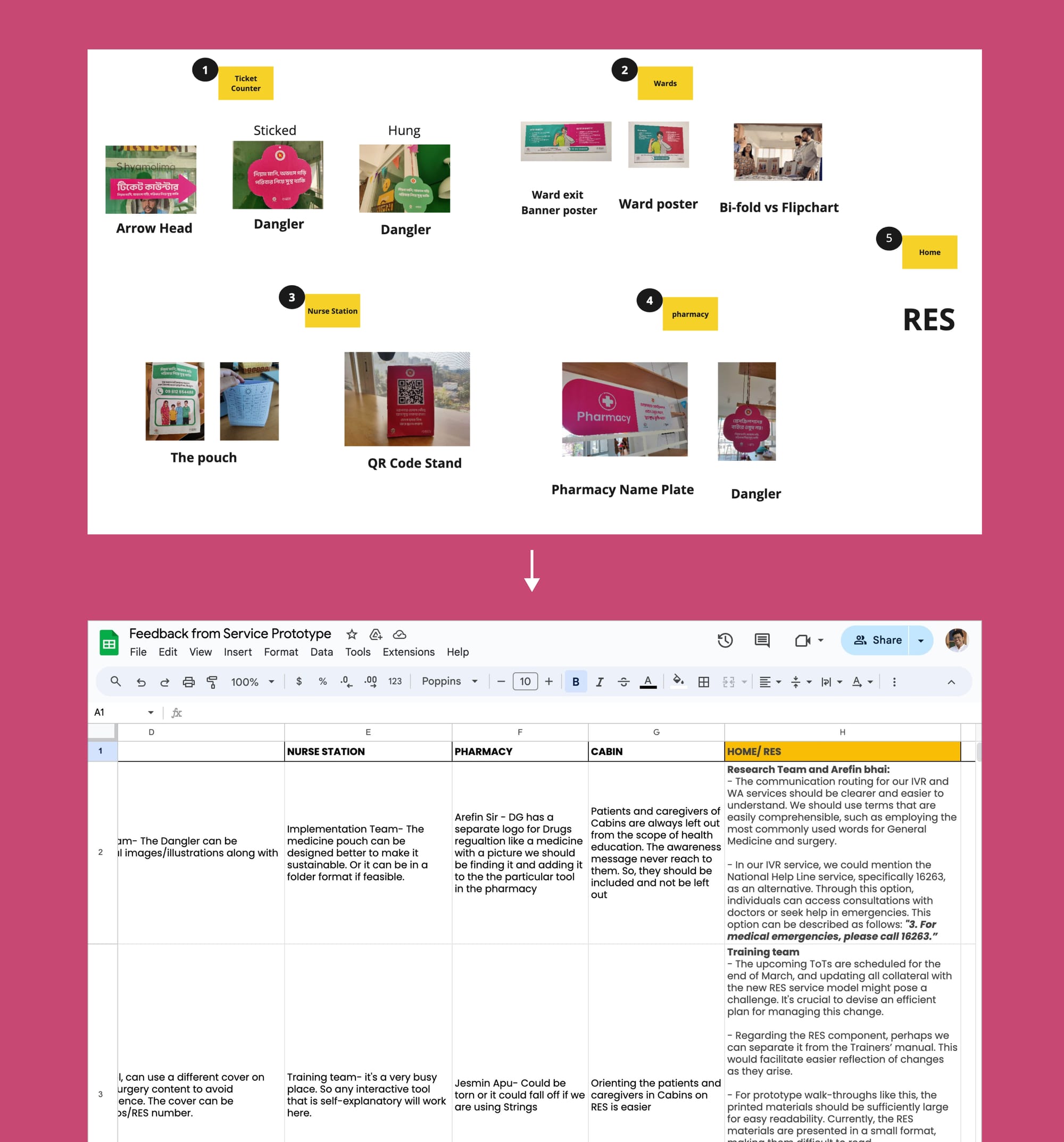
Incorporating Feedback—Aligning stakeholders along the whole process was the most challenging part of this process. To solicit timely and relevant input from stakeholders, it was crucial to present them with the appropriate artefacts at the right level of fidelity. Overly detailed artefacts might deter critical feedback, while overly vague ones might not provide enough substance for meaningful commentary. We used one pagers, concept notes, mockups, and sometimes even service prototypes to gather feedback
Beyond simple concept notes, we often found it more effective to simulate the entire user journey through a walkthrough. This approach transformed the experience into an interactive role-play rather than just a static document, making the feedback process more engaging and insightful.
One Pagers — Sometimes showing a prototype might feel like too much effort was put into its production that some stakeholders might avoid providing harsher feedback. They might feel that it's already well formed, and any critical comments would probably not be incorporated. To avoid this barrier, concept notes/one-pagers come in handy.
Medium Fidelity Prototypes — When I usually build the case around the opportunity, and have to start from zero, momentum is gained with a medium-fidelity prototype. By putting an idea out there, even if it's totally wrong is much better catalyst for getting to a good solution as people are more likely to react to an idea than to nothing. Prototypes were a great source of enquiry. Prototyping was also my super-power and used my personal conviction to fuel the development of such prototypes.
Imagine Rabeya's relief at receiving bite-sized WhatsApp lessons perfectly tailored to her needs as a new parent. Or the reassurance of having a supportive voice just a call away, ready to guide her through those inevitable anxious moments. For her, RES Bangladesh became a trustworthy companion on one of life's most profound journeys.
But the true measure of our success lies not in metrics, but in the countless lives touched.
In parents empowered with knowledge.
In preventable complications avoided.

In the smiles of healthy children born into a brighter future.
{kind=link}
World's most ancient public health problem
Maternal mortality rates have remained stubbornly static over the past 8 years, and in some countries, from the United States to Venezuela, they have risen.
From the place I come from, in Kerala, a baby is not given a name until he/she is 28 days old. And for marginalised castes/communities, the naming ceremony is delayed to 90 days. I never really questioned as to why this was the case. I let it become a ritual system until I overheard a conversation between some of our family members. This was mainly because the chances of a baby surviving was very low in our previous times. So our forefathers temporarily delayed the naming ceremony to avoid the emotional downpour if things go south. And for marginalised communities, the mortality rate was even more low owing to the difficult circumstances.
Knowing this reality shocked me. We might have more complex challenges facing the world right now — AI taking people’s jobs, climate change induced shock waves, food insecurities, refugee rights, future pandemics etc. But I believe that the cause of addressing maternal deaths requires the most urgency. When a mother dies during childbirth, the future dies with her.
This death happens 800 times a day. Worldwide. Once every two minutes, a mother dies from complications due to childbirth.
By the time you would have finished reading this introduction, there might have been a few maternal deaths.
It’s a remarkable irony that we’re still way off when it comes to maternal mortality rate. Even despite breakthrough progress in wide range of global challenges. AIDS medicines, contraceptives, bed nets to prevent malaria, childhood vaccines, even Tuberculosis for that matter.
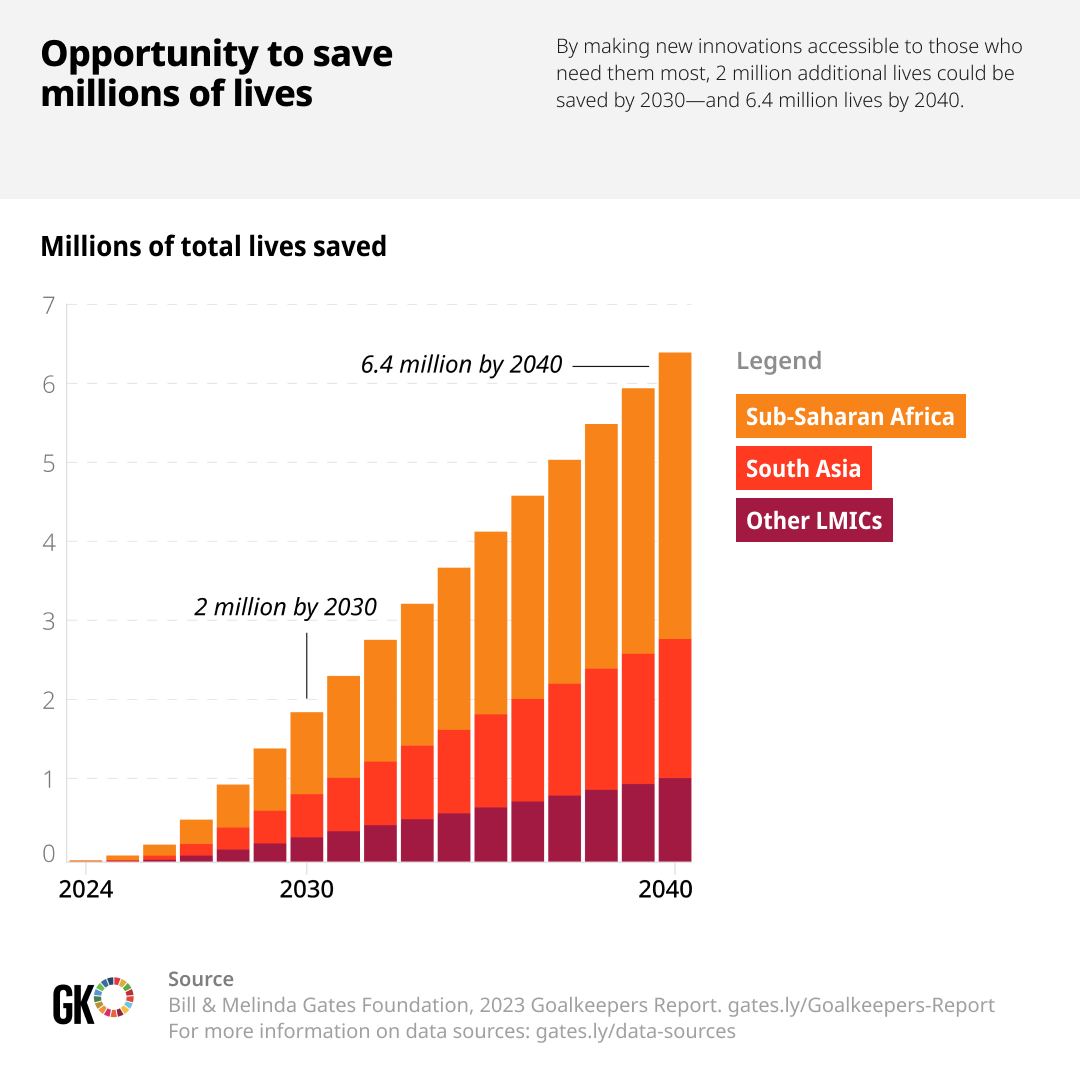
If you notice the figure below, you’ll only see a 3% annual decline from 2000. We’re way off the SDG target of reaching less than 70 deaths per 100,000 live births.
It’s also a strange problem as it’s not just solved by overall economic development of the respective country. Globally, maternal mortality rates have remained stubbornly static over the past eight years, and in some countries, from the United States to Venezuela, they have risen. 2
Let that sink in a bit. United States has seen a surprising rise in their MMR post COVID. The death rates of black mothers in UK and US have doubled since 1999. There is a huge opportunity for all of us to save millions of lives. If we are able to make more innovations accessible to the LMIC countries, almost 6.4 million lives could be saved by 2040.
We need innovations of all forms to tackle this. Not just technical innovations, but we need systemic innovations too. At Noora Health, we understand the power of health education training, and how that could have a profound impact for parents and their families. Our way of tackling this challenge has been through the systemic front.


An example of how we do service walkthroughs at Noora Health
By providing the right information at the right time, the curriculum is able to help new parents and their loved ones navigate this journey. For newly delivered mothers, it could be the first days for a newborn. For an expectant mother, it could be during the entire antenatal period.

Once a patient is discharged from the hospital, it’s the family who takes care of them. By imparting health education to the family, various risks are avoided. We want to tap into this unlimited resource. This, to us, is a systemic innovation as the desire to help people we love is universal.
The Care Companion Program (CCP) model at Noora Health is uniquely designed around a set of principles that are known to promote behavior change, but aren’t often implemented and rarely in combination:
- Family Centered, engaging the family member vs. the patient who is often exhausted and trying to recover;
- Timely, providing caregivers what they need when they need it;
- Trust-Based, anchoring on healthcare staff who families trust,
- Skills Oriented, focusing on equipping families with actionable skills that drive health outcomes;
- Reinforcing, supporting caregivers throughout their journey from the hospital to home, not just at one time.
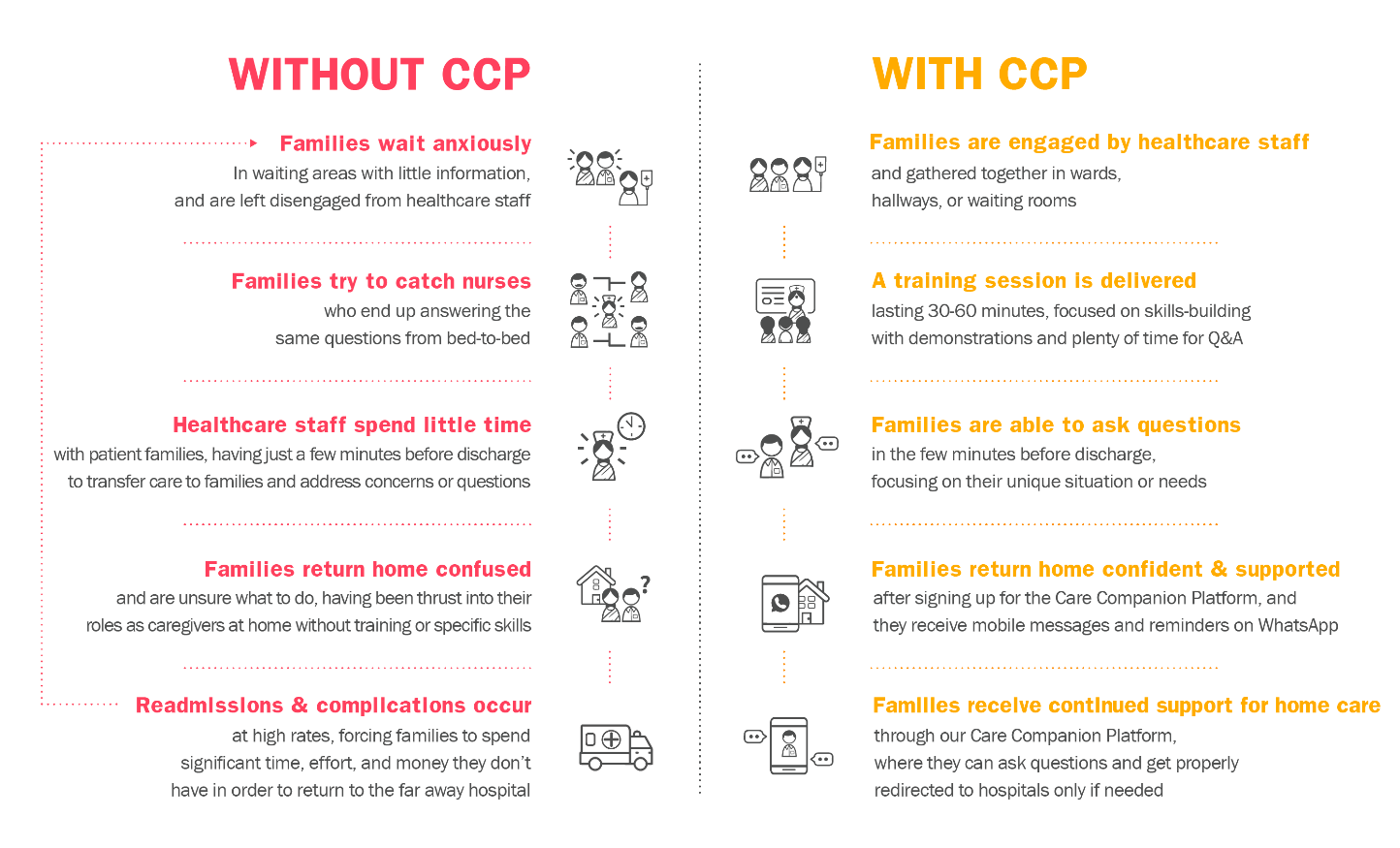

After leaving healthcare facilities, caregivers have access to the Noora-managed Care Companion Platform, which helps reinforce and supplement the skills and information received. Caregivers sign-up at the hospital, and then receive tailored information at scheduled points in time, including reminders and new content, most often via WhatsApp.
The Platform also provides on-demand support. Caregivers can ask questions that are fielded by Noora’s clinical team of nurses, who either clarify or supplement behavior change advice (e.g., steps for wound care, diet advice for diabetics), or provide advice on when symptoms warrant a healthcare facility visit.
While this level of support may seem daunting to provide at scale, 95% of the questions received can be answered from a bank of Frequently Asked Questions and only 5% require escalation to our team of doctors and specialists.
In this way, by looking at health education through a more systemic lens, we’re able to provide crucial information for the caregivers at each and every phase of their journey.